Acute Human Parvovirus B19 Infection an Immunocompetent Female Adult: A Case Report
ABSTRACT
Acute human Parvovirus B19 infection is a well-known cause of infectious erythema in pediatric age. However, in adult patient clinical picture is different but characteristic presenting with erythema, acute polyarthritis, systemic inflammation, hepatic enzymes elevation and anemia. Here, we present a case report about a nonpregnant immunocompetent adult female with a compelling symptom and a serological confirmation also a suspected close epidemiological contact was an infant with infectious erythema. We describe the clinical spectrum of this infection. To recognize its clinical picture and laboratory abnormalities, as well as the infant as a close contact, should make the clinician consider acute human parvovirus B19 infection as main differential diagnosis.
KEYWORDS
Human Parvovirus B19; Arthritis; Infectious erythema
CASE REPORT
A 33-year-old women was admitted as inpatient complaining 3-day fever, malaise, headache, myalgia and nausea. For two days, she started right knee and left ankle pain, with limitations for movements and then bilateral elbow, wrist and metacarpophalangeal pain and edema with complete movement limitation (Figure 1). Also, she noted macular erythema involving her abdomen, torso thighs and arms. She also passed 3 liquid stools.
Her past medical history was unremarkable, except for a close contact with her 2-year-old nephew who suffered a febrile illness associated with exanthema (Figure 2) She didn’t mention any mosquito’s bites.
Her vital signs were normal, she was eutrophic and alert. There was no alopecia, 0.5cm posterior cervical nodes were palpable, conjunctival injection was noted., there were no oral ulcers. Cardiopulmonar examination was unremarkable. In the abdomen there were no hepatomegaly nor splenomegaly.
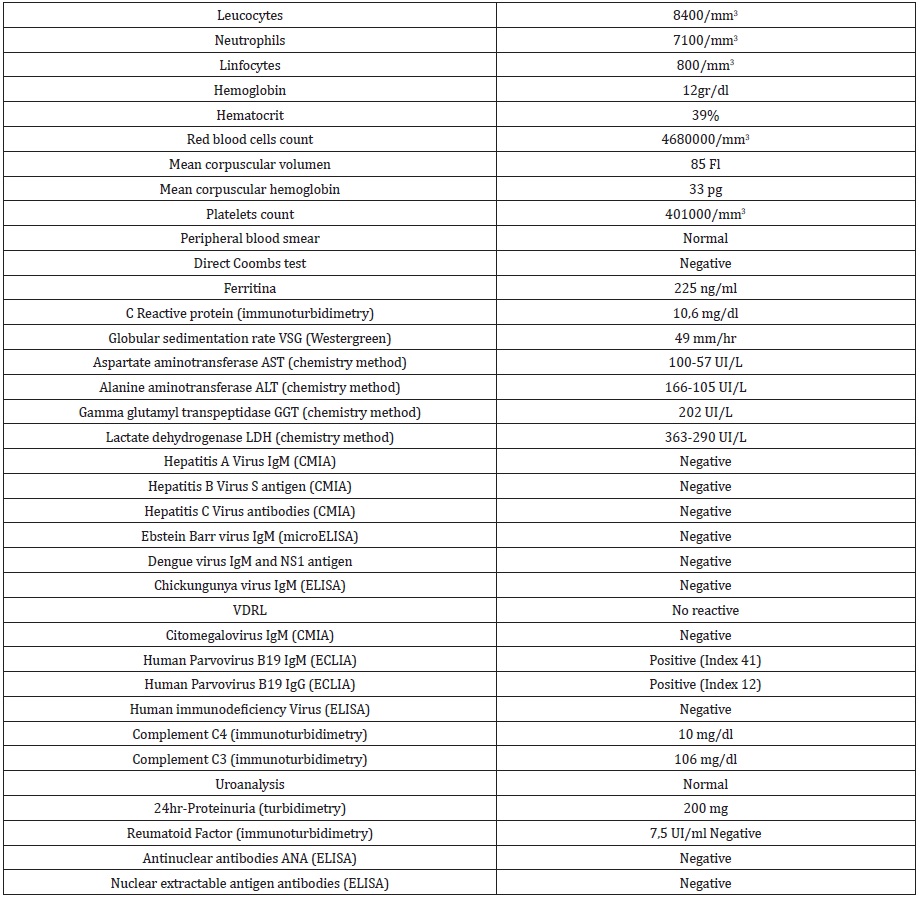
Extremities pains were elicited when elbow, wrist and metacarpophalangeal joints were palpated. Pain was also evident when passive joint movement. There were no tenosynovitis. Skin showed erythematous and confluent macular lessions in abdomen, back, arms and thighs. There were no pruritus signs and no purpuric rash (Figure 3). There were no vaginal discharge. She was evaluated by Internist, who considered judging by the clinical picture involving fever, rash and polyarthritis the first diagnosis was a viral origin acute polyarthritis. Laboratory blood sample were taken including complete blood count, inflammatory reactants, and basic biochemistry were taken. Also, autoimmune and viral serology were ordered and acute Parvovirus B19 infection was made as definite diagnosis (Table 1).
Two weeks after discharged the patient recovered uneventfully. She was given oral nonsteroidal anti-inflammatories and prednisolone 10 mg; this medication was suspended after one week. She developed carpal tunnel syndrome 2 months later.
REVIEW
Parvovirus B19 is a DNA virus belonging Parvoviridae virus family and Erythroviridae genera. Widespread geographical distribution and human infections is presented sporadically or in clusters [1]. Human is the only known host and its transmission occurs by respiratory secretions (common in schools and kindergarten) but transplacentary and hemocomponents routes has been also described.
Clinical presentation varies depending on the host. In children infectious erythema is the main clinical picture also known as “fifth illness” with slapped cheeks-; in adult patient arthralgia and arthritis is the most frequent clinical manifestation [2]; in pregnant women fetal anemia, nonimmune fetal hydrops and intrauterine death and in immunocompromised patients or who suffer chronic hemolysis pure erythroid aplasia is the clinical picture. Other clinical involvement described in literature has been encephalitis, peripheral nerve, hepatitis and myopericarditis [1,2].
Acute Parvovirus B19 infection is frequent. However, is rare and probably underdiagnosed in adult patient because nonspecific symptoms [3]. Mean age of presentation is from 30s to 40s in women predominantly, in 50% of cases a close contact with an infant with fifth illness can be documented. As in the case we presented above, fever, arthralgia and arthritis can be seen in 75% of cases, also erythematous macular rash, lynfopenia with anemia which resolves in less than 2 weeks in 75% of the cases, increased acute inflammatory reactants and liver enzymes elevation in 87% of patients [4]. Sometimes peripheral nerve involvement remains as sequela, as was in our case report [5]. In immunocompetent host diagnosis can be confirmed with positive serologic IgM test for Parvovirus [6].
CONCLUSION
As a conclusion, in adult otherwise healthy patient presenting with fever, acute polyarthritis, anemia or leucopenia, inflammation and increased liver enzymes and close contact with a suspected infant with “fifth illness”, acute Parvovirus B19 infection must be considered between differential diagnosis.
ETHICAL CONSIDERATIONS
The Hospital Universitario SanVicente Fundacion Ethical and Research Committee approved the Case Report by Act 19-2021. Also the patient and the parents of the case contact read, understood and signed the Informed Consent to publish the case.
REFERENCES
- Torné J, Blanch J, Garcia X, Baucells JM (2008) Parvovirus B19 infection in immunocompetent adult patients. Med Clin (Barc) 130(2): 78.
- Drago F, Ciccarese G, Agnoletti AF, Cogorno L, Muda A, et al. (2015) Remitting seronegative symmetrical synovitis with pitting edema associated with parvovirus B19 infection: two new cases and review of the comorbidities. Int J Dermatol 54(10): e389-393.
- Lavoipierre V, Dellyes A, Aubry C, Zandotti C, Lafforgue P, et al. (2016) Acute polyarthritis in a young patient caused by meningococcal and parvovirus B19 infections: a case report and review of the literature. J Med Case Rep 10(1): 362.
- Drago F, Semino M, Rampini P, Rebora A (1999) Parvovirus B19 infection associated with acute hepatitis and a purpuric exanthem. Br J Dermatol. 141(1): 160-161.
- Musiani M, Manaresi E, Gallinella G, Zerbini M (2007) Persistent parvovirus b19 infection resulting in carpal tunnel syndrome. J Clin Pathol 60(10): 1177-1178.
- Korman AM, Alikhan A, Kaffenberger BH (2017) Viral exanthems: An update on laboratory testing of the adult patient. J Am Acad Dermatol 76(3): 538-550.
Article Type
Case Report
Publication history
Received date: July 27, 2021
Published date: October 01, 2021
Address for correspondence
Carlos José Atencia Flórez, University of Antioquia, Colombia; ORCID 0000-0002-4531-229X
Copyright
©2021 Open Access Journal of Biomedical Science, All rights reserved. No part of this content may be reproduced or transmitted in any form or by any means as per the standard guidelines of fair use. Open Access Journal of Biomedical Science is licensed under a Creative Commons Attribution 4.0 International License
How to cite this article
Atencia C, Quintero C. Acute Human Parvovirus B19 Infection an Immunocompetent Female Adult: A Case Report; ORCID 0000-0002-4531-229X. 2021- 4(5) OAJBS.ID.000325.
Figure 1: Articular manifestations.

Figure 2: Cutaneous manifestations.

Figure 3: Infant close contact in recent days with the patient. Slapped cheeks can be noted.

Table 1: Laboratory blood test of the case, IgM, Immunoglobulin M. IgG, Immunoglobulin G. VDRL, Venereal Disease, Research Laboratory. ELISA, Enzyme linked immunosorbent assay. CMIA, Chemiluminescent microparticle enzyme immunoassay. ECLIA, Electrochemioluminiscent immunoassay.