Unusual Low-Grade Spindle Cell Sarcoma Pattern of Dedifferentiation Occurring in Chondrosarcoma: A Case Report
INTRODUCTION
Chondrosarcoma is a cartilage forming tumour, typically found in flat bones such as the ilium. It is known to have a male preponderance and encountered in the older age group. The lesions are locally aggressive, and onset of symptoms is gradual. Dedifferentiated chondrosarcoma typically has 2 microscopic components, whereby the low-grade cartilaginous lesion is seen with a high grade sarcomatous component with an abrupt transition between the 2 zones [1]. This pattern of dedifferentiation occurs in about 10% of chondrosarcomas [2,3]. The femur is involved in about 30% of these lesions and majority of the tumors are seen beyond the sixth decade [1]. We report an unusual pattern of dedifferentiation occurring in a chondrosarcoma where the pattern of dedifferentiation was that of a low-grade spindle cell sarcoma.
CASE PRESENTATION
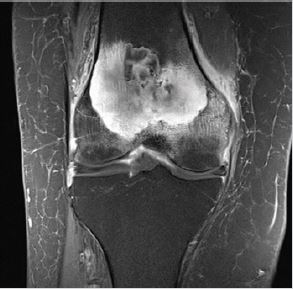
A 90 yr. old female presented with increasing hip and knee pain over the past 6 months. She was initially assessed by a physician who had obtained routine radiographs of the hip, which were normal. CT scans of the hip and knee were carried out. The hip images were normal, and the knee images demonstrated features of a large lytic lesion with endosteal scalloping and areas of calcification. The features were suggestive of a benign lesion and are shown in Figure 1 below. An MRI scan was arranged which showed periosteal reaction on the medial and lateral sides with endosteal scalloping and 2 distinct areas within the lesion. The features were consistent with a locally aggressive low-grade sarcoma with no breach in the femoral cortex and are shown in Figure 2 below.
After a detailed discussion with our specialist team, it was decided to perform an open biopsy of the knee. The procedure was performed under image intensifier control and the histological picture of the specimen showed features of a dedifferentiated lowgrade chondrosarcoma with abrupt demarcation between a distinct cartilaginous component and a spindle cell component. The biopsy showed evidence of a low grade chondroid neoplasm with features indistinguishable from enchondroma associated with a surrounding low grade fibrous proliferation, which invaded into marrow spaces. Although dedifferentiation in a chondrosarcoma was strongly considered, the pattern was considered unusual and the possibility of a collision tumor (enchondroma with desmoplastic fibroma) was also entertained, with recommended treatment to achieve control of a locally aggressive neoplasm.
Surgical enbloc resection of 6cm of the distal femur was carried out followed by Stryker hinge total knee arthroplasty. The Implant and surgical reconstruction are shown in Figure 3 below. The gross specimen of the distal femur had areas of calcification with the 2 components of the tumor well visualized. The entire metaphyseal region and most of the epiphyseal region was occupied by the tumor mass with central portions of the lesion showing a grey-blue cartilaginous appearance. Histological features were consistent with a dedifferentiated chondrosarcoma. There were central nodules of hyaline cartilage showing a minor increase in chondrocyte cellularity and rare binucleate forms. This component merged abruptly with a surrounding spindle cell component which widely infiltrated medullary spaces and into the overlying bone cortex. The spindle cell component consisted of short intersecting fascicles with storiform areas. The nuclei were ovoid with even chromatin pattern and minimal pleomorphism. Scattered mitotic figures were noted and the pattern resembled a low grade myofibroblast sarcoma. The findings indicated a dedifferentiated chondrosarcoma. The patient was progressing well at 3 months post operatively, walking with minimal support and had 100 degrees of flexion at the knee. She was followed up regularly in our outpatient clinic and continued to function well with good ROM, knee function and independence. Three years later she died having undergone no further surgery to the knee.
DISCUSSION
Chondrosarcomas are known to be the third most common malignant tumour occurring in bone and constitutes approximately 20% of primary bone sarcomas [3]. These tumours are rarely seen in the young patients (3). Secondary change occurs following malignant transformation of primary benign lesions such as an enchondroma and most of these are slow growing. Chondrosarcomas are graded according to the degree of cellular atypia and anaplasia [1-3]. The factors differentiating low grade and high-grade tumours are the cell density, amount of matrix, pleomorphism, presence of mitotic activity and binucleation (3).
Dedifferentiation of a low-grade chondrosarcoma is thought to occur when a high-grade sarcoma develops within the locally aggressive lesion [1]. Almost 30% of the dedifferentiated tumor have been encountered in the femur [1]. Patients typically present with recent onset of pain in an area of long-standing discomfort. This may be associated with swelling or fullness. Pathological fracture occurs in about 50% of these tumors at presentation. The radiological features suggestive of this lesion are areas of popcorn calcification which are typical features of a chondrosarcoma with poorly defined lytic areas and loss of bony architecture. A chest x-ray and bone scan are essential to rule out metastases. MRI is helpful to define the exact extent of the lesion, soft tissue component if present, and adequate preoperative planning. An open biopsy gives the histological picture and the various treatment options, prognosis can be discussed with the patient and relatives.
The typical microscopic pattern in majority of these lesions consists of a highly malignant spindle cell component coexistent with a low-grade chondrosarcoma [2,4]. The low-grade cartilaginous lesion and a rapidly emerging high-grade component are clearly demarcated [1,3]. The 2 components of the tumor are usually well demarcated on gross examination. The case presented herein is notable because of the low-grade pattern of dedifferentiation. The spindle cell component had no microscopic evidence of a highgrade sarcoma with only mild cellular atypia and scattered mitotic figures.
The literature indicates that this pattern of dedifferentiation is recognized, but rare. One report of 26 patients with dedifferentiated chondrosarcomas demonstrated that the second component in all tumors were highly anaplastic mesenchymal spindle cell sarcomas with histological features of lesions such as malignant fibrous histiocytoma, osteosarcoma and rhabdomyosarcoma [4]. However, 2 of their cases had a low-grade spindle cell pattern of dedifferentiation similar to the findings presented in the current case [4].
CONCLUSION
In summary, the microscopic findings in our case featured an unusual combination of a low-grade chondrosarcoma with dedifferentiation to a low-grade spindle cell component. It has been reported that no recurrences occur in selected low-grade chondrosarcomas after conservative surgical treatment [5,6], however, dedifferentiated chondrosarcomas with a high-grade sarcoma component have poor prognosis and the survival rate at 1 year is less than 10% [5,6]. Conservative surgical treatment was not the best option in our case taking into consideration the age of the patient and the nature of the lesion. Distal femur resection and hinge knee arthroplasty was carried out as an ablative procedure to ensure wide resection and improved rehabilitation time.
REFERENCES
- Dorfman HD (1998) Malignant cartilage tumors. Missouri, USA.
- Unni KK, Inwards CY, Bridge JA, Kindblom LG, Wold LE (2005) Tumors of the bones and joints. ARP Press, Washington, USA.
- Greenspan A, Jundt G, Remagen W (2007) Differential diganosis of orthopaedic oncology, Lippincott Williams & Wilkins, Philidelphia, USA.
- Johnson SB, Tetu AG, Chawla SP (1986) Chondrosarcoma with additional mesenchymal component (dedifferentiated chondrosarcoma). I. A clinicopathologic study of 26 cases. Cancer 58(2): 278-286.
- Souna BSN, Belot HD, Langlais F, Thomazeau H (2010) No recurrences in selected patients after curettage with cryotherapy for grade I chondrosarcomas. Clin Orthop Relat Res 468(7): 1956-1962.
- Weber KL, Raymond AK (2002) Low-grade/dedifferentiated/high-grade chondrosarcoma: A case of histological and biological progression. Iowa Orthop J 22: 75-80.
Article Type
Case Report
Publication history
Received Date: January 07, 2022
Published: January 20, 2022
Address for correspondence
Christopher John Wilson, Consultant Orthopaedic surgeon and Director of arthroplasty research, Flinders University and Flinders Medical Centre, Australia
Copyright
©2022 Open Access Journal of Biomedical Science, All rights reserved. No part of this content may be reproduced or transmitted in any form or by any means as per the standard guidelines of fair use. Open Access Journal of Biomedical Science is licensed under a Creative Commons Attribution 4.0 International License
How to cite this article
Christopher JW. Unusual Low-Grade Spindle Cell Sarcoma Pattern of Dedifferentiation Occurring in Chondrosarcoma: A Case Report. 2022- 4(1) OAJBS.ID.000380.