The Preventions of Dental Caries in Children - A Short Scoping Review
ABSTRACT
Background and Objective: The main theme of this article is to discuss the preventions of dental caries/ reasons and causes
of the dental caries in children-A short scoping review.
Methods: The Author of this article has chosen scoping review methodology of 22 random research articles about the
preventions of dental caries in children. 22 Articles were reviewed to prove the theme that what are the top 10 reasons/ causes
for the dental caries in children. 22 Articles also discussed in the tables as frequency for the top 10 interventions to prevent dental
caries in the children. Different way of data presentation and data collection is also discussed in the scoping review of different
authors and different countries, ethnicity and culture among the children around the globe.
Results: The author of the article has presented two tables and two SPSS Diagrammatic data analysis. Table 1 is about 22
websites & journal articles discusses about 10 interventions for the protection of dental caries in children Anil 2017. Table 2
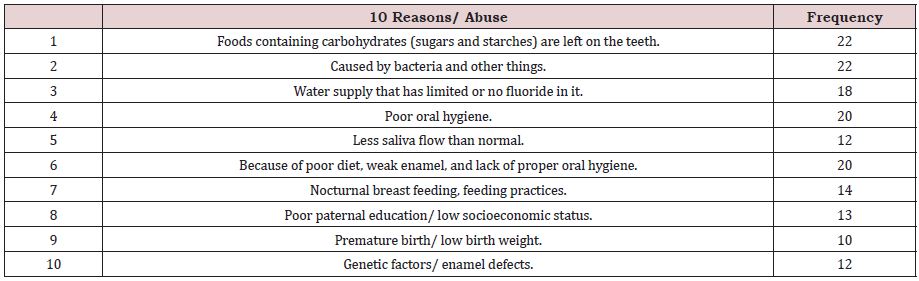
discusses 22 websites & journal articles discusses about 10 reasons/ abuse for the dental caries in children (Kids health 2021). Two
SPSS diagrams show the data analysis of the 10 reasons and 10 preventions of the dental caries in the children.
Conclusion: To conclude, the author has presented the reasons mostly our children have developed the dental caries in
childhood. The author has also given the preventions to treat the dental caries among our children. The Scoping review discusses
the community of children around the globe and their habits which develops the dental caries and found out common habits in all
children. Parents education is a must for the oral hygiene of the children and proper food rich in fluoride/drinks to control the dental
caries among children.
KEYWORDS
Children; Dental caries; Eating habits; Middle East; Northern Africa; Oral health; Risk factors; Socioeconomics; Sugar intake; Tooth brushing; Caries incidence; Down’s syndrome; caries prevalence; trisomy 21; Prevention; Diagnosis; Detection; Risk assessment
INTRODUCTION
Dental caries was found to be high among children in many [1] of the studies published from MENA. The key determinants of dental caries were found to include factors related to child characteristics family background oral hygiene and infant feeding and eating habits. The high dental caries prevalence emphasizes the need to address the prevailing modifiable socio behavioral and socioeconomic determinants by translating them into effective oral health prevention policies and programs. A total number of 369 Egyptian children and adolescents (age ranges from 3-18 years) were examined over the period from 15th November 2017 to 13th January 2018. Socio-demographic data oral hygiene measures and dietary habits for children were recorded. Dental status was analyzed using decayed missing and filled tooth index (DMFT) for deciduous dentition and (DMFT) index for permanent dentition. In primary dentition DMFT of the children was positively correlated with age beans, candies, crackers, chocolates and inversely correlated with gender socio-economic status (SES) [2] parental education brushing frequency of the parent brushing frequency of the parent to the child teeth.
A total of 164 articles were entered the meta-analysis [3]. The prevalence of dental caries in primary teeth in children in the world with a sample size of 80,405 was 46.2% (95% CI: 41.6- 50.8%), and the prevalence of dental caries in permanent teeth in children in the world with a sample size of 1,454,871 was 53.8% (95% CI: 50-57.5%). Regarding the heterogeneity on the basis of meta-regression analysis there was a significant difference in the prevalence of dental caries in primary and permanent teeth in children in different continents of the world. With increasing the sample size and the year of study dental caries in primary teeth increased and in permanent teeth decreased.
Overall, the model fit was adequate [4]. No alcohol consumption of the mother after giving birth higher frequency of child drinking sugar-sweetened beverages emotional and behavioral difficulties of the child and being male were directly associated with both BMI and dental caries. Caregivers uninvolved or indulgent feeding style were associated with higher BMI and less dental caries. Fifteen indirect paths were significant for both child dental caries and BMI. The findings suggest common determinants for both childhood obesity and dental caries. Common risk factor approach seems appropriate for planning future health promotion programs.
Dental caries appears prevalent and is socially distributed in Australia [5]. Policy efforts should consider how to ensure that children with dental caries receive adequate prevention and early care with equitable uptake. The odds of dental caries were higher for children with lowest vs. highest SEP (adjusted OR (adjOR) 1.92, 95% CI 1.49–2.46), and lower where water was fluoridated to recommended levels (adjOR 0.53, 95% CI 0.43–0.64). There was no evidence of an association between caries experience and either reported sugary diet or tooth brushing.
METHODS
The Author of this article has chosen scoping review methodology of 22 random research articles about the preventions of dental caries in children. 22 Articles were reviewed to prove the theme that what are the top 10 reasons/ causes for the dental caries in children. 22 Articles also discussed in the tables as frequency for the top 10 interventions to prevent dental caries in the children. Different way of data presentation and data collection is also discussed in the scoping review of different authors and different countries, ethnicity and culture among the children around the globe.
Dental caries was prevalent among children [6]; (83%, 95% confidence interval 79.7-86.0%). Individual factors including irregular brushing late adoption of brushing habit consulting dentist for symptomatic treatment lack of breast feeding sleeping with a bottle in mouth habit of snacking between meals low consumption of fruits and frequent consumption of soft drinks and flavored milk were predominantly associated with dental caries in children instead of socioeconomic factors (p< 0.05, adjusted R-square 80%).
Risk factors for dental caries have been identified and a caries [7] prediction model has been developed for Saudi pre-school children. The prediction mode if verified may provide with guidance in identifying high caries risk Saudi preschool children as targets for preventive programs. There was a highly significant difference between the two groups in debris index (P< 0.0001), aged child started tooth brushing, (P<0.0001), age breastfeeding was stopped (P< 0.005), nocturnal bottle feeding with milk formula (P<0.001), use of sweetened milk (P< 0.0001), frequency of use of soft drinks (P< 0.0005), frequency of consumption of sweets (P< 0.0001), and age at first dental visit (P< 0.0001).
Dental caries is a common public health problem in school children [8] associated with poor oral hygiene dietary and dental visit habits. Therefore, prevention measures such as health education on oral hygiene dietary habits and importance of dental visit are obligatory for children. Of the 147 children 82 (55.4%) were girls. Majority of the children (67.6%) cleaned their teeth using traditional method (small stick of wood made of a special type of plant). The proportion of children having dental caries was 32 (21.8%). Primary tooth decay accounted for 24 (75%) of dental caries. The proportion of missed teeth was 7 (4.8%).
We found that five studies have reported a higher prevalence [9] of Dental Caries among the Down syndrome-DS population. Three studies reported that there was no difference in the Dental Caries prevalence among the DS population when compared to those without DS. The findings of these studies emphasize the need to prioritize preventive and curative programs for this special care group. Oral health education programs should focus on targeting the DS population as well as their caretakers in order to help them in achieving better quality of life.
Measure and Statistical Analysis
(Table 1,2 & Figure 1,2); [10,11]
RESULTS
The author of the article has presented two tables and two SPSS Diagrammatic data analysis. Table 1 is about 22 websites & journal articles discusses about 10 interventions for the protection of dental caries in children [10]. Table 2 discusses 22 websites & journal articles discusses about 10 reasons/ abuse for the dental caries in children [11]. Two SPSS diagrams show the data analysis of the 10 reasons and 10 preventions of the dental caries in the children.
Caries prevalence was associated with several [12] behavioral and socioeconomic factors including screening site maternal employment toothbrushing duration past dental treatment, and past emergency visit. Efforts should be made to address these factors to minimize barriers and improve oral health behavior and care utilization. These findings can be used to evaluate current public health initiatives and inform future planning. Among 1000 first-grade children 78.0% had decay in their primary teeth with a mean DMFT of 3.7. Among 934 seventh-grade children 48.2% had caries in their permanent teeth with a mean DMFT of 1.7.
The prevalence of dental caries was found to be high [13] among 3- to 5-year-old preschool children and caries experience increased with age. This was mostly associated with sugar consumption and therefore calls for educational interventions to control sugar intake. The toothbrushing habit is well established in Khartoum State Sudan as a large number of children were found to be brushing their teeth regularly. No significant association was found between feeding habits and DMFT score. Dental caries has a significant impact on the general health [14] and development of children. Understanding caries epidemiology is an essential task for the United Arab Emirates (UAE) policymakers to evaluate preventive programs and to improve oral health. The purpose is to collect and summarize all data available in the published literature on the epidemiology of dental caries in the UAE in children aged under 13 years. This will provide dental health planners with a comprehensive data summary which will help in the planning for and evaluation of dental caries prevention programs. Data were collected from the various published studies in PubMed Academic Search Complete Google and the reference lists in relevant articles.
DISCUSSION OF PREVENTIONS
Protective factors which include salivary calcium phosphate [15] and proteins salivary flow and fluoride in saliva can balance prevent or reverse dental caries. Fluoride works primarily via topical mechanisms which include (1) inhibition of demineralization at the crystal surfaces inside the tooth (2) enhancement of remineralization at the crystal surfaces (the resulting demineralized layer is very resistant to acid attack) and (3) inhibition of bacterial enzymes. Fluoride in drinking water and in fluoride-containing products reduces tooth decay via these mechanisms. Low but slightly elevated levels of fluoride in saliva and plaque provided from these sources help prevent and reverse caries by inhibiting demineralization and enhancing remineralization.
Universal optimum application of fluoride and substitution [16] of starchy foods for sugary ones (or even simply judicious consumption of sugar) would alone do most of the job. Sealing of susceptible occlusal areas with adhesive polymers promises to protect the sites where fluoride evidently cannot be maximally effective. It seems unlikely that any single measure will be found sufficient to control this multifactorial disease. Anticaries food additives and antibacterial agents for intraoral use seem to be approaching practicability.
We found that supervised regular use of fluoride mouth rinse by children [17] and adolescents is associated with a large reduction in caries increment in permanent teeth. We are moderately certain of the size of the effect. Most of the evidence evaluated use of fluoride mouth rinse supervised in a school setting but the findings may be applicable to children in other settings with supervised or unsupervised rinsing although the size of the caries‐preventive effect is less clear.
Caries progression or reversal is determined by the [18] balance between protective and pathological factors. Fluoride the key agent in battling caries works primarily via topical mechanisms inhibition of demineralization enhancement of remineralization and inhibition of bacterial enzymes. Fluoride in drinking water and in fluoride-containing products reduces caries via these topical mechanisms. Antibacterial therapy must be used to combat a high bacterial challenge.
Despite the attractions of targeting cost-effective prevention [19] should be aimed first at the whole population with more expensive activities targeted to all children in a chosen geographic area rather than to individually selected children. In the Scandinavian countries the prime population strategies are the regular use of fluoride toothpaste and public education that emphasizes oral hygiene. Fluoride varnish and sealants though effective is expensive and need careful selection of locality and teeth to be efficient. With the recent shift from the surgical model which emphasized [20] restorative treatment to a medical model of disease management newer strategies emphasizes disease prevention and conservation of tooth structure. For early detection and monitoring of caries rather than waiting until a cavity is formed and restorative treatment is needed devices such as DIAGNOdent Digital Imaging Fiber-Optic Transillumination quantitative lightinduced fluorescence and the Electronic Caries Monitor have been introduced. For caries prevention oral hygiene measures fluoride application pit-and-fissure sealants the use of xylitol the development of a dental caries vaccine and the role of the primary caregiver for infants are briefly discussed.
The laser diagnosis system makes it easy to detect the [21] existence of caries under a pit and fissure sealant during a routine check-up. The mean reflected fluorescence value was significantly decreased by chemical irrigation. The reflected fluorescence value before and after sealants was tested for statistical significance. The diagnosis of caries under sealants was up to 10 of reflected fluorescence value in the study. Clear and red sealants were used to reveal caries under sealants using visual inspection and all sealants’ groups achieved 90% of reflected fluorescence value after sealants application.
Laser can be used as a suitable alternative to many [22] conventional diagnostic and therapeutic dental procedures. It is especially efficient for caries detection and removal pulp therapy lowering the risk of infection inflammation and swelling and reducing bleeding. Laser technology has been recently introduced into the dental field with the idea to replace drilling. Pedodontics need to learn the new less invasive technologies and adopt them in their routine practice.
The prevalence of dental caries in children and adults [23] in the United States has been declining the past 40 years primarily because of increased use of fluoride improved oral hygiene and better oral hygiene devices a greater emphasis on disease prevention and control and better access to dental care made available by the dental profession. In recent years a number of new technologies have become available as adjuncts to traditional methods of diagnosing carious lesions. Caries prevention has traditionally relied on fluoride [24] exposure diet control thorough oral hygiene and antibacterial measures. Prevention of caries as an NCD does certainly not disqualify these methods but brings them into a new context. Besides the established routines of regular toothbrushing with fluoride products there is an opportunity for additional technologies based on ecological principles to address and modify the oral biofilm. Biofilm engineering through pre and probiotics early in life to support microbial diversity seem promising in order to obtain a sustained caries-preventive effect [25].
CONCLUSION
To conclude, the author has presented the reasons mostly our children have developed the dental caries in childhood. The author has also given the preventions to treat the dental caries among our children. The Scoping review discusses the community of children around the globe and their habits which develops the dental caries and found out common habits in all children. Parents education is a must for the oral hygiene of the children and proper food rich in fluoride/ drinks to control the dental caries among children.
REFERENCES
- Amal E, Malin G, Anzelle M (2021) Determinants of dental caries in children in the Middle East and North Africa region: a systematic review based on literature published from 2000 to 2019. BMC Oral Health 21(1): 237.
- Marwa A, Sara M, Sara EM Dina R, Nermen A, et al. (2019) The prevalence of dental caries among Egyptian children and adolescences and its association with age, socioeconomic status, dietary habits and other risk factors. A cross-sectional study. F1000Res 8: 8.
- Mohsen K, Alireza A, Shamarina S, Rostam J, Aliakbar V, et al. (2019) Dental caries in primary and permanent teeth in children’s worldwide 1995 to 2019: a systematic review and meta-analysis. Head Face Med 16(1): 22.
- Magdalena U, Sarah B, Peter D (2021) Common determinants of dental caries and obesity in children: A multi-ethnic nested birth cohort study in the United Kingdom. Int J Environ Res Public Health 18(23): 12561.
- Sharon G, Kate F, Monsurul H (2019) The impact of policy modifiable factors on inequalities in rates of child dental caries in Australia. Int J Environ Res Public Health16(11): 1970.
- Yazeed A, Abdulhameed A, Nagarajkumar Y, Hoda J (2018) Prevalence of dental caries and associated factors among primary school children: a population-based cross-sectional study in Riyadh, Saudi Arabia. Environ Health Prev Med 23(1): 60.
- Ghanim NA, Adenubi JO, Wyne AA, Khan NB (1998) Caries prediction model in pre-school children in Riyadh, Saudi Arabia. Int J Paediatr Dent 8(2): 115-122.
- Wondemagegn M, Tazebew D, Mulat Y Kessaw M, Bayeh A (2014) Dental caries and associated factors among primary school children in Bahir Dar city: a cross-sectional study. BMC Res Notes 7: 949.
- H Ashi (2021) Dental caries experience among down’s syndrome population in Saudi Arabia-A systematic review. Niger J Clin Pract 24(8): 1109-1116.
- Anil S, Anand PS (2017) Early childhood caries: prevalence, risk factors and prevention. Front Pediatr 5: 157.
- Kids health (2021) Keeping your child’s teeth healthy.
- Hosam A, Ahmid E, Reema B (2021) Prevalence of dental caries and associated factors among school-aged children in Tripoli, Libya: a crosssectional study. BMC Oral Health 21(1): 224.
- Sitana ME, Sudeshni N (2016) Prevalence of dental caries and toothbrushing habits among preschool children in Khartoum State, Sudan. Int Dent J 66(4): 215-220.
- Ghada SM (2014) Epidemiology of dental caries in children in the United Arab Emirates. Int Dent J 64(4): 219-228.
- John DBF (2007) Prevention and reversal of dental caries: role of lowlevel fluoride. Community Dent Oral Epidemol 27(1): 31-40.
- Henry WS (1971) Dental caries: prospects for prevention: Combined utilization of available and imminent measures should largely prevent this ubiquitous disease. SCIENCE 173(4003): 1199-1205.
- Marinho VCC, Chong LY, Worthington HV, Walsh T (2016) Fluoride mouth rinses for preventing dental caries in children and adolescents. Cochrane Database Syst Rev 7: CD002284.
- John DBF (2000) The science and practice of caries prevention. J Am Dent Assoc 131(7): 887-899.
- Brian AB (1998) Prevention policies in the light of the changed distribution of dental caries. Acta Odontol Scand 56(3): 179-186.
- Lee Y (2013) Diagnosis and prevention strategies for dental caries. J Lifestyle Med 3(2): 107-109.
- Takamori K, Hokari N, Okumura Y, Watanabe S (2001) Detection of occlusal caries under sealants by use of a laser fluorescence system. J Clin Laser Med Surg 19(5): 267-271.
- Nazemisalman B, Farsadeghi M, Sokhansanj M (2015) Types of lasers and their applications in pediatric dentistry. J Lasers Med Sci 6(3): 96- 101.
- Strassler HE, Sensi LG (2008) Technology-enhanced caries detection and diagnosis. Compound Contin Educ Dent 29(8): 464-470.
- Svante T (2018) Prevention of dental caries as a non-communicable disease. Eur J Oral Sci 126(1): 19-25.
- SPSS 20 (2021) IBM SPSS Software.
Article Type
Mini Review
Publication history
Received Date: March 7, 2022
Published: March 16, 2022
Address for correspondence
Ahsan Ali Siddiqui, Assistant Professor Family Medicine, Ministry of Health Saudi Arabia, Saudi Arabia
Copyright
©2022 Open Access Journal of Biomedical Science, All rights reserved. No part of this content may be reproduced or transmitted in any form or by any means as per the standard guidelines of fair use. Open Access Journal of Biomedical Science is licensed under a Creative Commons Attribution 4.0 International License
How to cite this article
Ahsan AS. The Preventions of Dental Caries in Children - A Short Scoping Review. 2022- 4(2) OAJBS.ID.000416.
Figure 1: SPSS diagram shows 22 websites & journal articles discusses about 10 interventions for the protection of dental caries in children [10].
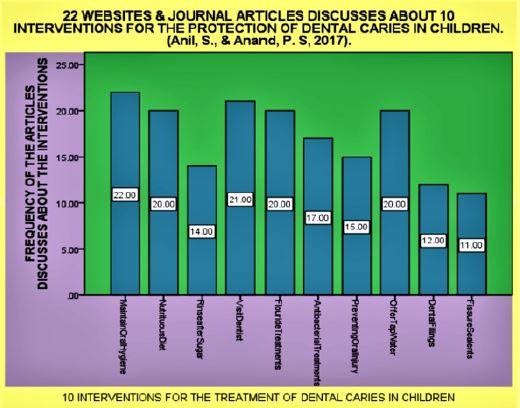
Figure 2: SSPSS diagram shows 22 websites & journal articles discusses about 10 reasons/ abuse for the dental caries in children [11].
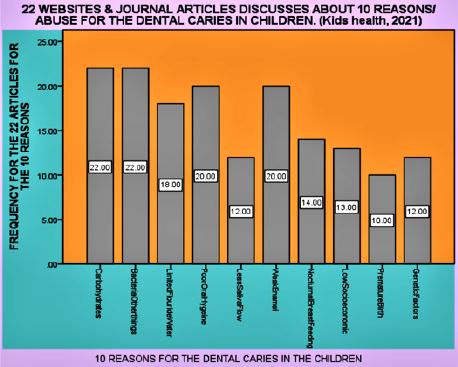
Table 1: 22 websites & journal articles discuss about 10 interventions for the protection of dental caries in children [10].
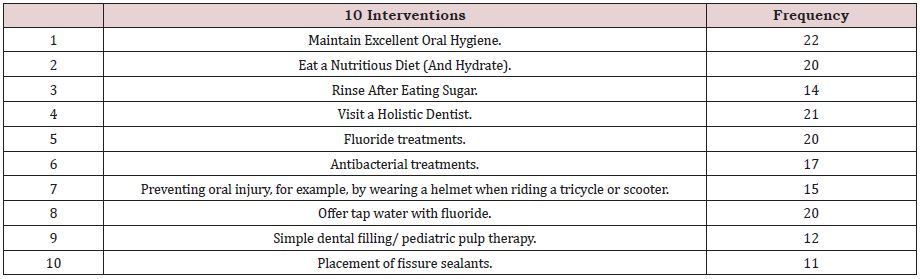
Table 2: 22 websites & journal articles discuss about 10 reasons/ abuse for the dental caries in children [11].