Rifaximin as an Alternative Treatment for Patients with Hepatic Encephalopathy
ABSTRACT
Introduction: Liver cirrhosis is the final stage of progressive chronic liver diseases. This is a histopathological alteration of the
liver that is characterized by the loss of the hepatic parenchyma, thus generating the formation of fibrous septa and structurally
abnormal regeneration nodules, thus giving rise to a distortion of the normal hepatic architecture and an alteration of the anatomy.
hepatic vasculature and microcirculation. Currently for the treatment of liver cirrhosis and its complications, there are different
drugs of which the main ones are lactulose, L-ornithine, L-aspartate (LOLA) and certain antibiotics, especially rifaximin.
Methodology: A bibliographic search was carried out in databases, selecting original articles, case reports and bibliographic
reviews from 2009 to 2021, using the documents that will deal with Rifaximin as an alternative treatment in hepatic encephalopathy,
obtaining 21 articles for the realization of this document
Results: In a 2015 meta-analysis, a significant comparison was made between the use of rifaximin and some other treatments
for HE, where it was shown that rifaximin has a greater reduction in plasma ammonium levels (which causes this complication).
studies comparing rifaximin with placebo, other antibiotics and non-absorbable disaccharide laxatives
Conclusion: IRifaximin is a dominant alternative in the treatment of acute episodes of hepatic encephalopathy and to prevent
its relapses
KEYWORDS
Rifaximin; Hepatic encephalopathy; Cirrhosis; Hepatic carcinoma
INTRODUCTION
Liver cirrhosis is the final stage of progressive chronic liver diseases. This is a histopathological alteration of the liver that is characterized by the loss of the hepatic parenchyma, thus generating the formation of fibrous septa and structurally abnormal regeneration nodules, thus giving rise to a distortion of the normal hepatic architecture and an alteration of the anatomy. of the hepatic vasculature and microcirculation. In the past, it was considered that cirrhosis was never reversible, however, in recent years the term cirrhosis has gone from being a static stage to a dynamic one. It is currently known that, by eliminating the fundamental aggression that has produced the cirrhosis, it could resolve the fibrosis; this can be seen in patients with hemochromatosis successfully treated with phlebotomies; patients with alcoholic liver disease in alcohol withdrawal; patients with cirrhosis of autoimmune etiology treated with immunosuppressants and chronic hepatitis C with cirrhosis stage with sustained virological response to antiviral treatment [1].
Liver cirrhosis is a very common pathology worldwide, and its prevalence varies between countries depending on etiological factors. Liver cirrhosis tends to manifest itself generally towards the fourth or fifth decade of life, however, there are cases of young people and even paediatrics, this pathology is a more frequent disease in males, probably because infection by viruses of hepatitis and alcoholism are more common in men. Black race, urban living, and low economic status appear to be significant risk factors for developing cirrhosis; The causes of cirrhosis are multiple, but approximately 90% of the causes of liver cirrhosis in Western countries are alcohol abuse. The complications that occur in liver cirrhosis are the same, regardless of the cause. This pathology is one of the main complications of decompensated cirrhosis and is involved in the appearance of ascites and bleeding from esophagogastric varices. In addition, hepatocellular dysfunction causes jaundice, coagulation disorders, and hypoalbuminemia and contributes to porto-systemic encephalopathy. Patients who develop complications of their liver disease and who become decompensated are candidates for liver transplantation. In addition, liver cirrhosis predisposes to the development of hepatocarcinoma [2].
Currently for the treatment of liver cirrhosis and its complications, there are different drugs of which the main ones are lactulose, L-ornithine, L-aspartate (LOLA) and certain antibiotics, especially rifaximin-(RFX); Rifaximin is an antibiotic with a broad spectrum of activity against bacteria, both gram-positive and gram-negative, and especially against anaerobic enteric bacteria. Its action is given by binding to the b subunit of RNA polymerase, which is dependent on DNA and prevents RNA synthesis. The little absorption at the intestinal level allows a high concentration in the gastrointestinal tract, therefore, the modification of the intestinal bacterial flora with blood levels of less than 1% after oral administration, for which Rifaximin is safe in healthy patients. Cirrhotic patients have an altered gut microbiota that could influence cognitive ability. The administration of antibiotics in hepatic encephalopathy is based on altering the bacterial flora and achieving a reduction in endotoxemia by reducing the production and absorption of neurotoxins derived from the intestine. By reducing the levels of ammonia and endotoxemia, a positive impact could be produced on the episodes of acute and chronic encephalopathy [3,4].
METHODOLOGY
To carry out this article, a bibliographic search was carried out in various databases such as Elsevier, Scielo, Medline, pubmed, ScienceDirect and Ovid, thus selecting original articles, case reports and bibliographic reviews from 2009 to 2021, in Spanish and English. using MeSH terms: rifaximin, hepatic encephalopathy, cirrhosis, hepatic carcinoma and Boolean operators and or. Thus, including all the documents that will deal with rifaximin as an alternative treatment in hepatic encephalopathy, the data found were between 18-32 records, thus using 21 articles to carry out this document.
RESULTS
Rifaximin is a broad-spectrum antibiotic used to treat hepatic encephalopathy (HE) secondary to liver cirrhosis and even used to prevent it. This entity affects approximately 30% to 50% of patients with liver cirrhosis. Rifaximin is a non-absorbable antibiotic that has been shown to be effective in the treatment of this complication [5]. It is an antibiotic with characteristics that give it greater tolerability than others such as lactulose, it is responsible for a marked decrease in the mortality of these patients (23.8% vs. 49.1%; p<0.05) and likewise a reduction in the hospital stay (5.8 +or- 3.4 days vs 8.2 +or- 4. it is used to assess a person’s perception of their health status with respect to the impact of their disease. It is sensitive enough to monitor changes in health status over time and is used to assess the effect of illnesses on physical and emotional functioning [6,7].
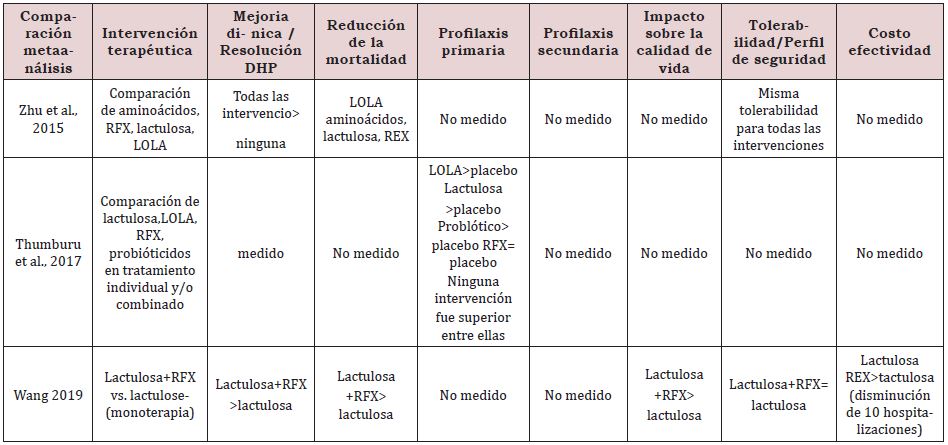
In a 2015 meta-analysis, a significant comparison was made between the use of rifaximin and some other treatments for HD, where it was shown that rifaximin has a greater reduction in plasma ammonium levels (causing this complication). studies comparing rifaximin with placebo, other antibiotics and non-absorbable disaccharide laxatives. In these studies, rifaximin has been shown to be equal to or better than different drugs when well tolerated when compared. Long-term studies have also been performed as maintenance therapy in comparison with non-absorbable disaccharides or neomycin. A study has recently been published comparing rifaximin with rifaximin maintenance therapy. The placebo group received free nonabsorbable disaccharides during the 2-year follow-up period. It shows a lower rate of recurrence of HE in patients treated with long-term rifaximin without major side effects being observed, also many recently published studies have shown that the role of rifaximin in the treatment of HE is more effective than disaccharides non-absorbable and other antibiotics used for the treatment of this, likewise it was reported that it had notorious beneficial effects in the prevention of acute episodes, in recurrence and in the management of minimal HE, in the same way the different reviews or meta-analyses suggest that rifaximin is at least as effective as the nonabsorbable disaccharide and that the latter is better tolerated. Nevertheless, it has not been found to be statistically superior. Therefore, international guidelines do not yet recommend its use as monotherapy for the treatment and prevention of recurrent episodes of HE (Table 1-3).
Rifaximin was more effective in lowering blood ammonia levels, resulting in fewer hospitalizations and length of stay, and savings in hospitalization costs. Treatment with non-absorbable disaccharide and rescue therapy with rifaximin has been shown to be cost-effective for those patients who initially did not respond to lactulose/lactitol, however, further studies are needed for this [8]. On the other hand, according to various European and American clinical practice guidelines on the management of HE, the best therapeutic options for the management of HE secondary to liver cirrhosis are management established with lactulose as the first line of treatment, rifaximin and salt of amino acids aspartate and ornithine (L-aspartate, L-ornithine or also called LOLA) also supported by the Mexican Association of Gastroenterology, considering lactulose as the first line followed by rifaximin and LOLA, however some guidelines such as the clinical practice guideline of Since 2013, the Mexican Secretary of Health continues to recommend the use of neomycin and metronidazole to patients who do not respond correctly to lactulose or lactitol, For this reason, in the study carried out by [9]. the evidence was reviewed against the efficacy of rifaximin compared to lactulose and others, in aspects such as efficacy in different degrees of HE, cost reduction, improvement in cognitive status, the efficacy in reducing and preventing patient falls and the improvement in their quality of life (Table 4-6); [9].
DISCUSSION
In cirrhosis, Rifaximin treatment in open hepatic encephalopathy is effective and well tolerated to reduce mortality and hospitalization to prevent hepatic encephalopathy recurrence and reduces subsequent hospitalizations; cures minimal hepatic encephalopathy and is profitable both in therapeutic aspects and in reduction of hospital costs, with positive economic results because it treats the same number of patients compared to other treatment alternatives, in a pharmaco-economic evaluation it showed that the combined rifaximin with lactulose is more effective and more cost-effective than other treatments against acute episodes of hepatic encephalopathy and for the prevention of its relapses. So, Metronidazole treatment has recently been compared with RFX in hepatic encephalopathy, it was based on patients with mild hepatic encephalopathy (grade I or II), evaluating the improvement after three days of treatment, there were no differences between rifaximin and metronidazole, but all received also lactulose, L-ornithine L-aspartate and enemas [10].
Rifaximin was also shown to be effective in improving survival in patients with cirrhosis in one study. A significant decrease in short-term mortality was seen for 10 days after treatment in patients who received lactulose plus rifaximin compared to patients who received lactulose alone [11] There are additional advantages of rifaximin treatment in patients with liver disease. Rifaximin treatment has been shown to prevent episodes of spontaneous bacterial peritonitis [12-14], as bacterial overgrowth in the small intestine in cirrhotic patients is common and associated with systemic endotoxemia, leading to worsening addition of portal hypertension. A recent meta-analysis found that rifaximin prevents episodes of spontaneous bacterial peritonitis compared to placebo and quinolone treatment [15] and also reduces the occurrence of hepatorenal syndrome [16]. In a study conducted in patients who had had hepatic encephalopathy without hepatocarcinoma, the rifaximin-lactulose combination compared to lactulose alone was associated with greater survival at 48 months, in addition to a decrease in complications, such as recurrent encephalopathy, bacterial peritonitis spontaneous and bleeding from oesophageal varices; in individuals with hepatocarcinoma, on the other hand, there was only a decrease in peritonitis [17].
A prospective study also showed that rifaximin reduces the levels of endotoxins, such as lipopolysaccharides, and improves systemic inflammation in cirrhotic patients. These data suggest that rifaximin may contribute to the control of intestinal microbiota imbalance and act as an important therapeutic agent to control bacterial overgrowth in the small intestine. These modulatory activities on the bacterial composition of the gut microbiota may underline the efficacy of rifaximin for gut-derived toxins that contribute to the development of complications of cirrhosis [18]. There are cost-effectiveness analyses of rifaximin-α for reducing episodes of open hepatic encephalopathy in the United Kingdom, France, and Italy. Treatment with RFX was considered cost-effective in all of them, with variable savings compared to standard treatment with lactulose, derived mainly from the decrease in hospitalization costs. This treatment increases quality-adjusted life years (QALYs) at an affordable cost [19,20].
CONCLUSION
It shows a lower rate of recurrence of HE in patients treated with rifaximin in the long term without major side effects being observed, in addition, in different patients, a significant decrease in short-term mortality was evidenced during 10 days after treatment in patients who received lactulose more rifaximin compared to patients who received lactulose, thus demonstrating that rifaximin is a dominant alternative in the treatment of acute episodes of hepatic encephalopathy and to prevent its relapses.
REFERENCES
- Buey GL, Gonzalez FM, Moreno OR (2012) Cirrosis hepática. servicio de aparato digestivo. Unidad de hepatología. Hospital universitario la princesa (IIS-IP). Madrid. España. Medicine11(11): 625-633.
- Lefton HB, Rosa A, Cohen M (2009) Diagnosis and epidemiology of cirrhosis. Med Clin North Am 93(4): 787-799.
- Cajamarca K (2020) Effectiveness of treatment with rifaximin and/or lactulose, aimed at reducing recurrence, mortality and hospitalizations in patients with hepatic encephalopathy. Cuenca: Catholic Ecuador.
- Sanchez J, Miquel M (2016) Role of rifaximin in the treatment of hepatic encephalopathy. Gastroenterología y Hepatología 39(4): 282-292.
- Torre A, Garcia S, Juarez F, Rodriguez H (2009) Guías de diagnóstico y tratamiento de la encefalopatía hepática, tratamiento y prospectivas a futuro. Rev Gastroenterol Mex 74(2): 170-174.
- Romero M, Sendra C, Ampuero J (2018) The impact of minimal hepatic encephalopathy treatment in long-term prognosis. Salud(i)ciencia (Impresa) 23(1): 34-42.
- Sidhu SS, Goyal O, Parker R, Kishore H, Sood A (2016) Rifaximin vs. lactulo- se in treatment of minimal hepatic encephalopathy. Liver Int 36(3): 378-385.
- Coronel C, Contreras J, Frati A, Uribe M, Mendez N (2020) Efficacy of rifaximin in the different clinical scenarios of hepatic encephalopathy. J Gastroenterio Mex 85(1): 56-68.
- Frati A, Galindo R (2020) Rifaximin-α in hepatic encephalopathy. Pharmaco-economic considerations for Mexico. Med Int Méx 36(5): 621-632.
- Mekky MA, Riad AR, Gaber MA, Abdel-Malek MO, Swifee YM (2018) Rifaximin versus metronidazole in management of acute episode of hepatic encephalopathy: an open labelled randomized clinical trial. Arab J Gastroenterol 19(2): 76-79.
- Sharma BC, Sharma P, Lunia MK, Srivastava S, Goyal R, et al. (2013) A randomized, double-blind, controlled trial comparing rifaximin plus lactulose whit lactulose alone in treatment of overt hepatic encephalopathy. Am J Gastroenterol 108(8): 1458-1463.
- Hanouneh MA, Hanouneh IA, Hashash IG, Law R, Esfeh JM, et al. (2012) The role of rifaximin in the primary prophilaxis of spontaneous bacterial peritonitis in patients with liver cirrhosis. J Clin Gastroenterol 46(8): 709-715.
- Shokoohi S, Zivony A, Le TD, Zaman A, Jou J (2013) Rifaximin is associated with decreased incidence of spontaneous bacterial peritonitis in cirrhotic with ascites. Hepatology 58: 858A Abst 1337.
- Kamal F, Kahn MA, Kahn Z, Cholankeril G, Hammad TA, et al. (2017) Rifaximin for the prevention of spontaneous bacterial peritonitis and hepatorenal syndrome in cirrhosis: a systematic review and metaanalysis. Eur J Gastroenterol Hepatol 29(10): 1109-1117.
- Ibrahim ES, Alsebaey A, Zaghla H, Abdelmageed SM, Gameel K, et al. (2017) Long-term rifaximin therapy as a primary prevention of hepatorenal syndrome. Eur J Gastroenterol Hepatol 29(11): 1247-1250.
- Kang SH, Lee YB, Lee JH, Nam JY, Chang Y, et al. (2017) Rifaximin treatment is associated with reduced risk of cirrhotic complications and prolonged overall survival in patients experiencing hepatic encephalopathy. Aliment Pharmacol Ther 46: 845-55.
- Vlachogiannakos J, Saveriadis AS, Viazis N, Theodoropoulos I, Foudoulis K, et al. (2009) Intestinal decontamination improves liver haemodynamic in patients with alcohol-related decompensated cirrhosis. Aliment Pharmacol Ther 29(9): 992-999.
- Berni E, Poole CD, Conway P, Radwan A, Currie CJ (2015) Cost effectiveness of rifaximin-A 550 mg (Xifaxan/Tagaxan) in the reduction of recurrence of overt hepatic encephalopathy. UEG journal 3(5S): A510.
- Berni E, Murphy D, Whitehouse J, Conway P, Di Maggio P, et al. (2018) Evaluation of the cost-effectiveness of rifaximina-α for the management of patients with hepatic encephalopathy in the United Kingdom. Curr Med Res Opin 34: 2001-2008.
- Roggeri DP, Roggeri A (2017) Economic impact of the use of rifaximin 550 mg twice daily for the treatment of overt hepatic encephalopathy. Hepat Med 9: 37-43.
Article Type
Mini Review
Publication history
Received Date: August 25, 2022
Published: November 30, 2022
Address for correspondence
Jose Dario OG, Universidad del Sinú, Spain, https:// orcid.org/0000-0001-6877-3227
Copyright
©2022 Open Access Journal of Biomedical Science, All rights reserved. No part of this content may be reproduced or transmitted in any form or by any means as per the standard guidelines of fair use. Open Access Journal of Biomedical Science is licensed under a Creative Commons Attribution 4.0 International License
How to cite this article
Jose Dario OG, Jesús David RGl, Paula Andrea RA, Eduard Orlando VP, Zaira Molina A, María del MM. Rifaximin as an Alternative Treatment for Patients with Hepatic Encephalopathy. 2022- 4(6) OAJBS.ID.000522.
Table 1: Rifaximin in the treatment of HE episodes [4].
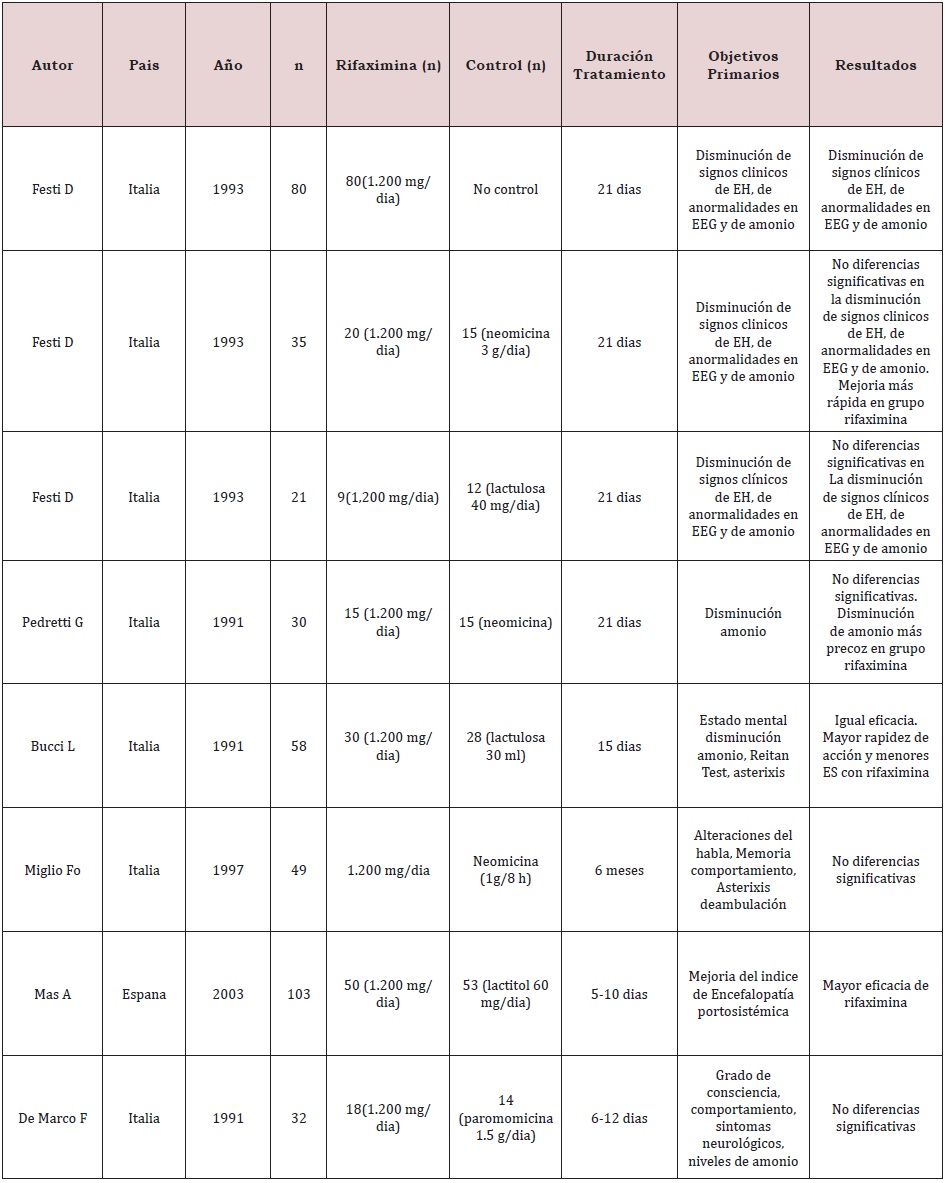
Table 2: Continued from Table1 [4].
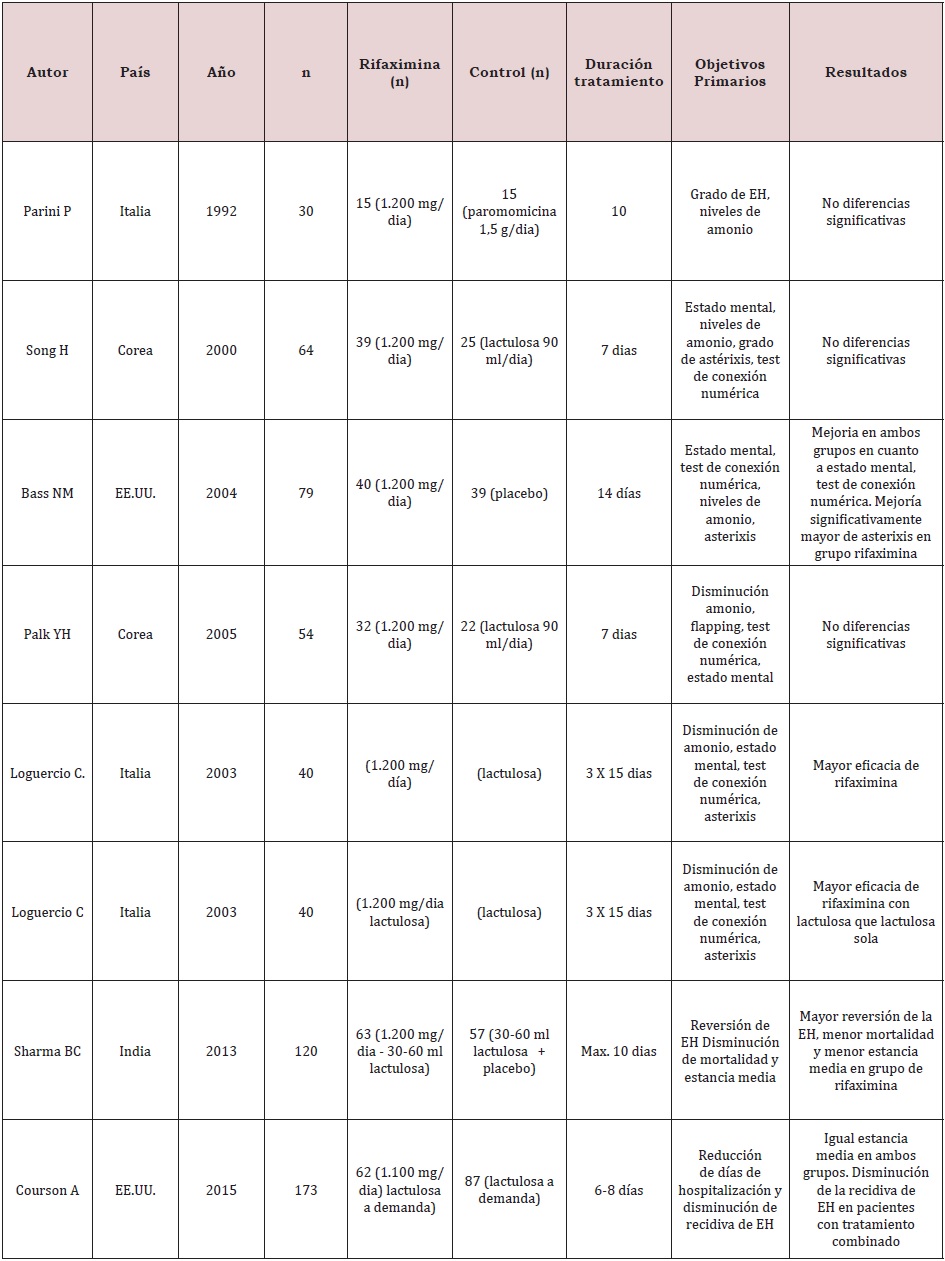
Table 3: Rifaximin in the prevention of HE recurrence [4].
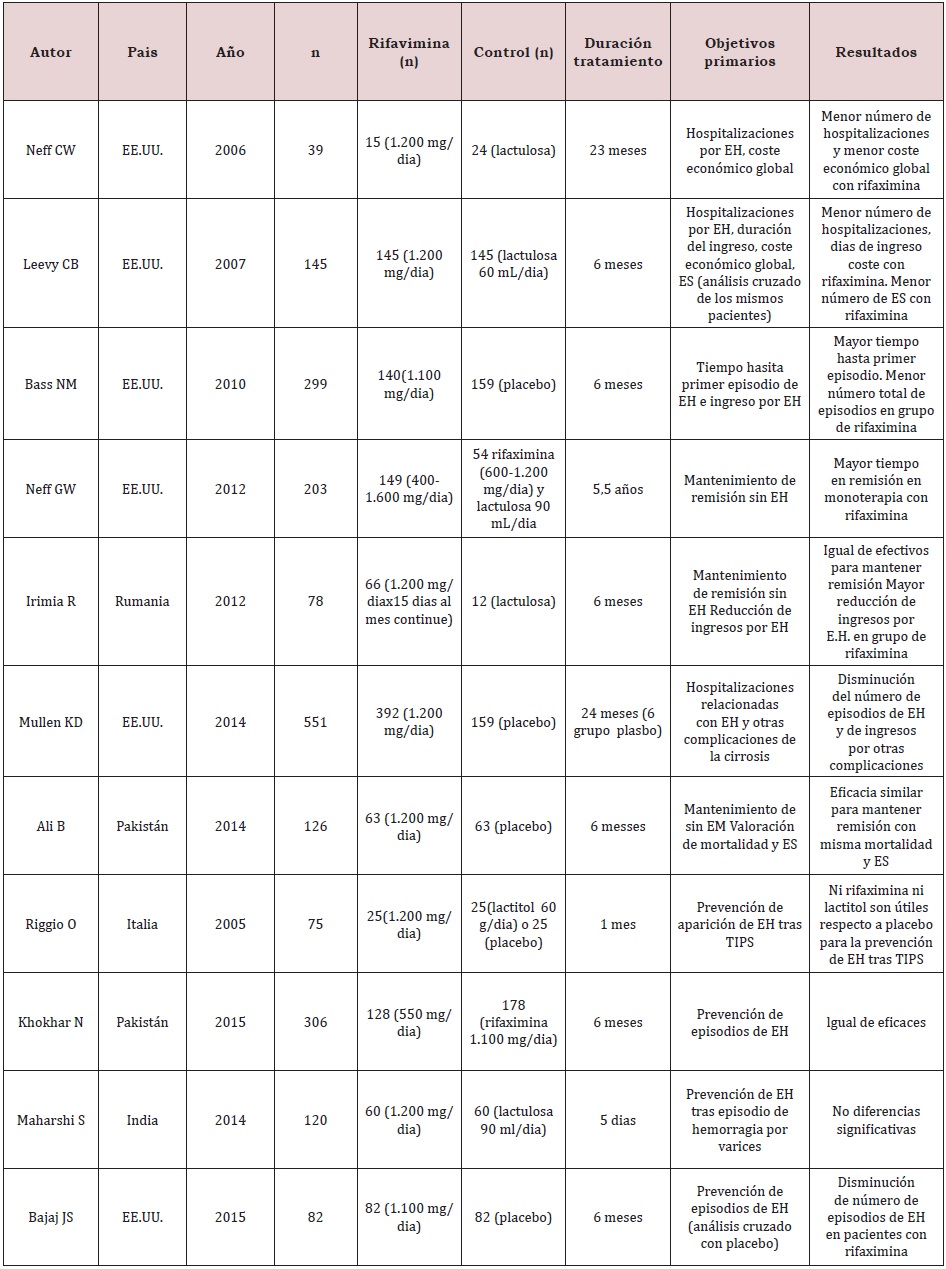
Table 4: Rifaximin in minimal HE [4].
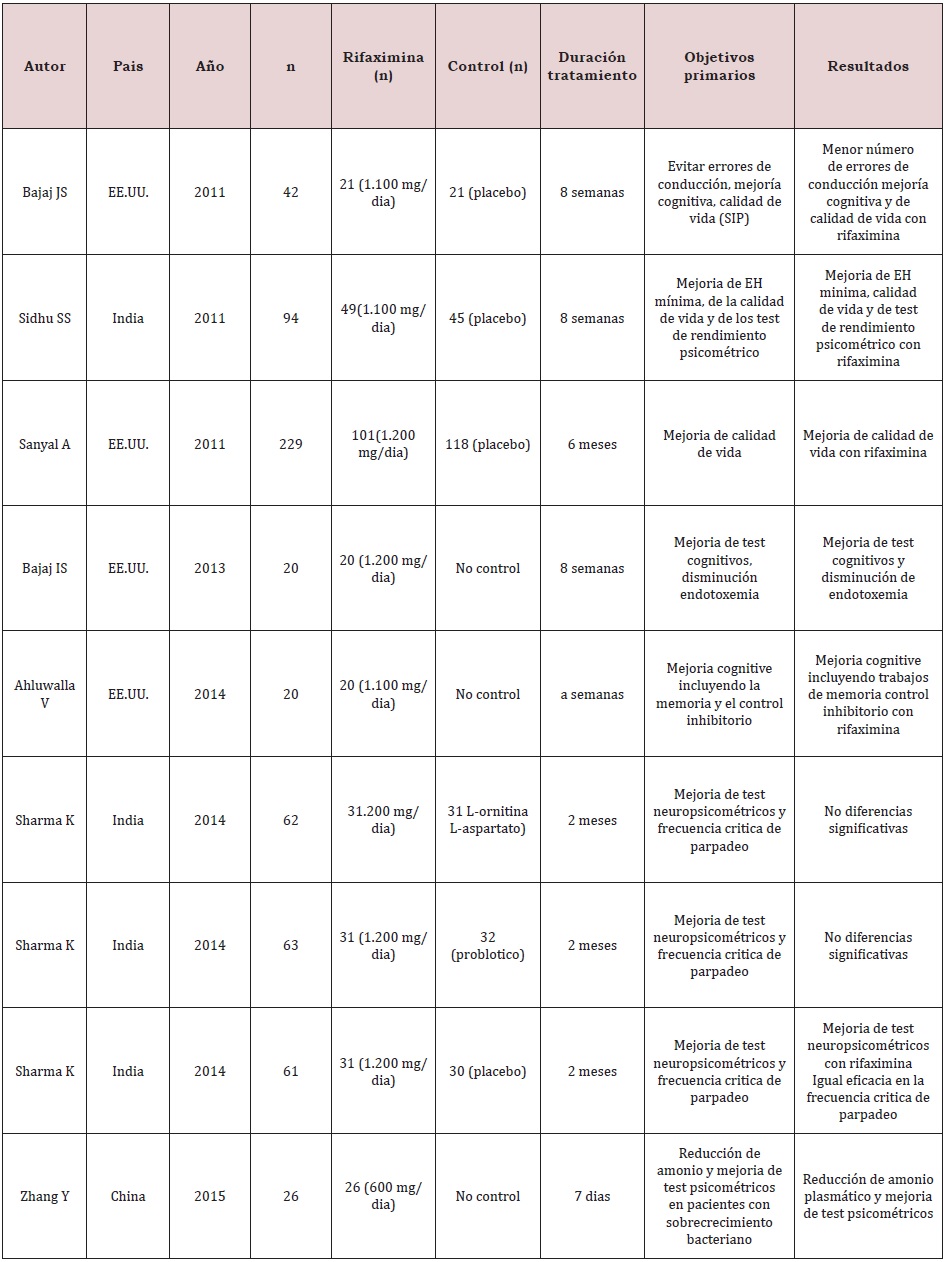
Table 5: Comparison of the efficacy of rifaximin in different variables of persistent HE [9].
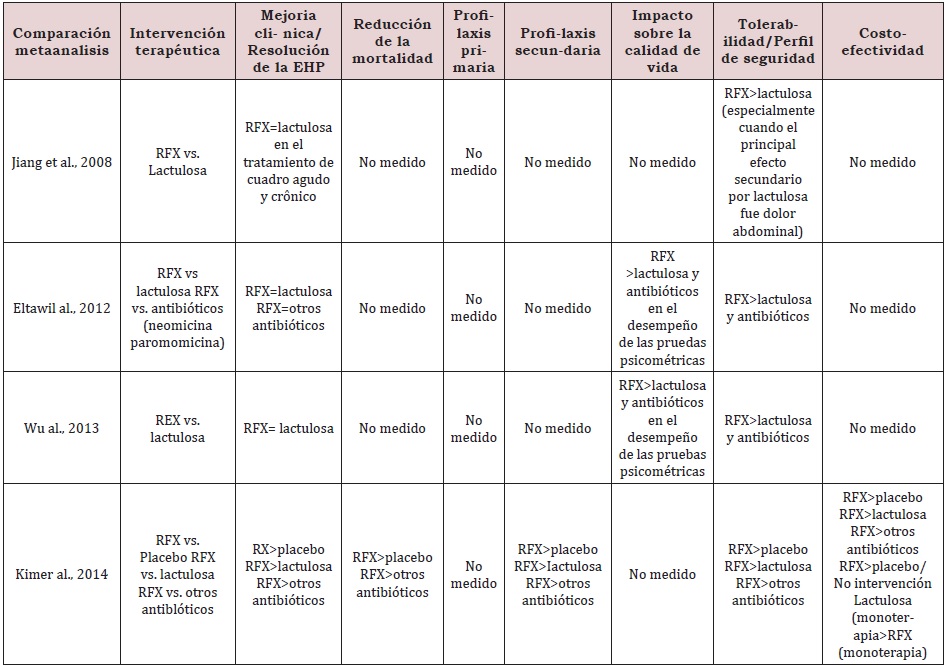
Table 6: Comparison of the efficacy of rifaximin in different variables of persistent HE (continuation from table 5), Taken from [9].