
Ribocyclib in the Treatment of Recurrent Low Grade Serous Ovarian Cancer: Case Report
ABSTRACT
Low grade serous ovarian cancer is one of the rare subtypes of epithelial-derived ovarian cancer. It differs from the more common, high grade serous carcinoma on a molecular and biological basis, has a different clinical course and a different response to the commonly used systemic treatment. Despite these differences, the standards of treatment for these two subtypes of ovarian cancer are the same - chemotherapy platinum-based regimens and bevacizumab - an anti-angiogenic drug are used. Due to the poor response to chemotherapy, new targets in treatment of low grade serous ovarian cancer (LGSOC) are currently being investigated. Because of the frequent presence of hormone receptors in this ovarian cancer subtype, currently are being tested potentially beneficial therapies with cyclin 4/6-dependent kinase inhibitors in combination with hormone therapy-it is a commonly used treatment for the metastatic, hormone-dependent, HER-2 negative breast cancer.g
KEYWORDS
Low grade serous ovarian cancer; Ribocyclib; Letrozol; CDK4/6 inhibitor
ABBREVATIONS
LGSOC: Low Grade Serous Ovarian Cancer; SOC: Serous Ovarian Carcinomas; HGSOC: High Grade Serous Ovarian Carcinoma; BOT: Borderline Ovarian Tumours
INTRODUCTION
Ovarian cancer is the second, after endometrial cancer, most common malignancy of the female gynaecological neoplasm and fifth in terms of cancer incidence in women. It is also leading gynaecologic cause of death [1]. Due to the non-specific symptoms, about 70% of these tumours are diagnosed in an advanced stage (FIGO III and IV). About 90% of ovarian malignant neoplasms are tumours of epithelial origin, the most common of which are serous ovarian carcinomas (SOC) [2]. There are two subtypes: subtype 1 - highly differentiated – Low Grade Serous Ovarian Carcinoma (LGSOC) and subtype - 2 low-differentiated – High Grade Serous Ovarian Carcinoma (HGSOC). LGSOC and HGSOC are thought to be disparate cancers, differing in the most common genetic mutations, disease course, prognosis, and response to chemotherapy [3]. The clinical case described below refers to a patient with low grade serous ovarian carcinoma, which tends to occur in younger patients, has a better prognosis and a longer median overall survival.
CASE REPRESENTATION
In September 2016 33-year-old woman was admitted to the hospital due to suspicion of a tubo-ovarian abscess. During hospitalization, an ultrasound of the abdominal cavity was performed, showing, in the midline of the body, below the navel, an area of heterogeneous reflections measuring 50 x 40 mm and a dense fluid space surrounded by thick walls approximately 59 x 58 mm in Douglas sinus - lesion described as an abscess. The patient was qualified for surgery, during which a disseminated neoplastic disease was found in the abdominal cavity - intraoperative histopathological examination was performed, after which it was concluded, that the reproductive organ is the most likely origin of the tumour. The greatest chances of long-term survival of patient were with optimal cytoreduction, so the procedure was extended according to the oncology protocol - the greater omentum, the uterus with the appendages were removed and, due to the presence of two tumours in the intestinal lumen, an anterior resection of the sigmoid colon and part of the rectum was performed with the exposure of an end colostomy on the descending colon. Finally, the FIGO IIIC ovarian cancer was diagnosed, in the histopathological examination it was a low grade psammomatic serum adenocarcinoma and in the immunohistochemical examination was found p16(+) in 50% of cells, p53(+) in 40% of cells, WT1(+) in 100% of cells, CEA (-), estrogen receptors in 80% of cells and progesterone in 50% of cells. Postoperative computer tomography revealed an abscess near the sinus of the sacrum, which was evacuated by transvaginal approach. In addition, CT revealed several focal liver lesions - the largest 29 mm on the border of segments 4b and 3, at the falciform ligament - which could correspond to meta lesions and a 20 x 15 mm epigastric calcified lesion. Accordingly, the stage of FIGO IVB disease was changed.
The patient received postoperative chemotherapy according to the paclitaxel 175 mg / m2 program with carboplatin AUC 5. After the first treatment course, another CT evaluation was performed, in which the fluid reservoir was still visible in the presacral region in connection with the rectal stump, as well as changes in the liver, the largest 21 mm and an epigastric implant. From the second course of chemotherapy, bevacizumab was added to the treatment. Due to the stabilization of the disease in the control CT examination - stable changes in the liver, reduction of the epigastric implant to 8 x 4 mm - it was decided to administer additional 2 courses of chemotherapy according to the paclitaxel-carboplatin regimen, up to a total of 8 courses. Subsequently, the patient continued bevacizumab maintenance treatment for 18 courses.
In another CT scan of the abdominal cavity and pelvis from December 2017, performed after the completion of first-line treatment, a partial remission of the neoplastic disease was found - complete withdrawal of the infiltrative lesion on the border of segments 4b and 3 of the liver and the absence of the epigastric lesion described above. The patient received a maintenance hormone therapy with an aromatase inhibitor - letrozole. She was under observation.
In the follow-up MR examination in August 2019, new lesions appeared that raised oncological concern: between the vaginal stump and the rectal wall on the left side 12 x 13 x 30 mm and in the left iliac fossa tangent to the lumbar muscle 12 x 11 x 20 mm. The patient was still under observation until October 2020, when the next MR revealed an enlargement of the previously described tumours - in the rectal area up to 48 x 35 x 48 mm with infiltration of the rectum and invagination into its lumen, with the left lumbar muscle up to 38 x 29 mm with tapping into the muscle and suspicion of its infiltration. Moreover, many implants were found in the abdominal cavity and pelvis, the largest size 30 x 13 mm in the distal attachments of the abdominal rectus muscles on the left side. Then the patient was qualified for the 2nd line treatment - paclitaxel at a dose of 80 mg / m2 with carboplatin AUC 2 administered weekly. Due to severe weakness and haematological toxicity, the dose of paclitaxel was reduced to 60 mg / m2 from the second course of treatment. In the control MR from January 2021, after 11 treatment courses, stabilization of the disease was found - a slight increase in the size of the lesion at the left lumbar muscle (up to 50 x 38 mm), the remaining lesions in the same number and size as before. The result did not meet the criteria for disease progression; therefore, the therapy was continued. During chemotherapy there was a complication as bleeding from the rectal stump treated conservatively and purulent inflammation of the rectal stump, which delayed the next treatment course. After antibiotic therapy and improvement in general condition, chemotherapy was continued. Control imaging tests - CT and MRI - showed stabilization disease after 18 treatment courses.
In April 2021, the patient started maintenance treatment with exemestane in combination with CDK 4/6 inhibitor - ribociclib. The patient tolerated the treatment well, and there were no side effects. At the next MR from August 2021, a regression of proliferative changes was found by RECIST1.1 criteria partial response was observed. Figure 1,2 show the radiological responses with this treatment regimen. Currently, the patient continues her treatment with good tolerance. The patient remains in a very good general condition, ECOG-0, with no symptoms of the disease. She works professionally.
DISCUSSION
LGSOC accounts for approximately 10% of serous ovarian cancers. It is more common in younger women, with an average age of onset of around 55 years (compared to 62 years for HGSOC) [4]. It can develop de novo or as a transformation of borderline ovarian tumours (BOT) [5]. Unlike HGSOC, these tumours are not associated with mutations in the BRCA gene and mutations in the TP53 gene are rare. The most frequently observed mutations include those in the KRAS, BRAF and NRAS genes [4,6]. Moreover, these tumours are more likely to express estrogen and progesterone receptors [7]. The most important prognostic factor is optimal debulking surgery [8]. Although LGSOC is characterized by a poor response to chemotherapy, the use of platinum-based regimens is standard practice in both adjuvant chemotherapy and the treatment of relapses [2]. Since most LGSOCs express steroid receptors (high ER expression seen in ~70% and high PR expression seen in ~30% cases), some patients may benefit from maintenance hormone therapy) [4]. In case of disease relapses, hormone treatment can lead to disease stabilization with relatively low toxicity. The possibilities of increasing the effectiveness of hormone therapy by adding cyclin 4/6 kinase inhibitors are currently being investigated [9]. The cyclin 4/6 dependent kinases in combination with the estrogen receptor regulated cyclin D1 play a key role in the transition from the G1 phase to the S phase of the cell cycle. Hormone therapy such as an aromatase inhibitor or fulvestrant in combination with CDK 4/6 inhibitors (palbociclib, ribociclib and abemaciclib) is successfully used in the treatment of metastatic hormone-dependent, HER-2 negative breast cancer and contributes to both the prolongation of progression free survival (PFS) and the confirmed prolongation of overall survival (OS) for ribociclib with relatively low toxicity [4,9].
Based on the results of clinical trials in the treatment of patients with hormone-dependent, HER2-negative breast cancer through the analogous potential of the combination of CDKi and aromatase inhibitors, the efficacy of ribociclib in combination with letrozole was assessed in a small phase II study [10] of ovarian and endometrial cancer patients (n = 40). Patients with LGSOC turned out to be the group that benefited most from this therapy - all 3 patients achieved long-term objective responses - one CR and two PR for over 2 years. The currently ongoing clinical trials that have a chance to bring new important data on this subject are two American studies: GOG 3026 (NCT03673124) - a phase II study with ribocyclib and letrozole, and NCT03531645, also phase II, assessing the effectiveness of fulvestrant and abemaciclib - both in patients with LGSOC [4].
CONCLUSION
The case of the patient described above confirms the effectiveness of such treatment also in the case of LGSOC - the patient has been receiving exemestane in combination with ribociclib for a 13 month with regression of neoplastic changes found in the control imaging examination, which could not be achieved with standard platinum-based chemotherapy. It is worth noting that the patient did not present any side effects of the treatment, did not require treatment breaks or dose reduction. This could present a potential therapeutic role of CDK4/6 inhibition in recurrent ovarian cancers.
CONSENT FOR PUBLICATION
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
AUTHOR CONTRIBUTION
Agnieszka Mlodzinska and Agnieszka Jagiello-Gruszfeld wrote the work. Anna Skrzypczyk-Ostaszewicz contributed to the revision of the work and gave the final approval of the version to be published. All authors read and approved the final manuscript.
REFERENCES
- Friedrich M, Friedrich D, Kraft C, Rogmans C (2021) Multimodal treatment of primary advanced ovarian cancer. Anticancer Res 41(7): 3253-3260.
- Konecny GE, Wang C, Hamidi H, Winterhoff B, Kalli KR, et al. (2014) Prognostic and therapeutic relevance of molecular subtypes in highgrade serous ovarian cancer. J Natl Cancer Inst 106(10): 249.
- Gockley A, Melamed A, Bregar AJ, Clemmer JT, Birrer M, et al. (2017) Outcomes of Women with High-Grade and Low-Grade Advanced-Stage Serous Epithelial Ovarian Cancer. Obstet Gynecol 129(3): 439-447.
- Moujaber T, Balleine RL, Gao B, Madsen I, Harnett PR, et al. (2021) New therapeutic opportunities for women with low-grade serous ovarian cancer. Endocr Relat Cancer 29(1): R1-R16.
- Kurman RJ, Shih IeM (2010) The origin and pathogenesis of epithelial ovarian cancer: a proposed unifying theory. Am J Surg Pathol 34(3): 433- 443.
- Pauly N, Ehmann S, Ricciardi E, Ataseven B, Bommert M, et al. (2020) Low-grade serous tumors: Are we making progress? Curr Oncol Rep 22(1): 8.
- Hacker KE, Uppal S, Johnston C (2016) Principles of treatment for borderline, micropapillary serous, and low-grade ovarian cancer. J Natl Compr Canc Netw 14(9): 1175-1182.
- Goulding EA, Simcock B, McLachlan J, van der Griend R, Sykes P (2020) Low-grade serous ovarian carcinoma: A comprehensive literature review. Aust N Z J Obstet Gynaecol 60(1): 27-33.
- Dall’Acqua A, Bartoletti M, Masoudi-Khoram N, Sorio R, Puglisi F, et al. (2021) Inhibition of CDK4/6 as therapeutic approach for ovarian cancer patients: Current evidence and future perspectives. Cancers (Basel). 13(12): 3035.
- Colon-Otero G, Zanfagnin V, Hou X, Foster NR, Asmus EJ, et al. (2020) Phase II trial of ribociclib and letrozole in patients with relapsed oestrogen receptor-positive ovarian or endometrial cancers. ESMO Open 5(5): e000926.
Article Type
Case Report
Publication history
Received Date: June 20, 2022
Published: July 01, 2022
Address for correspondence
Agnieszka Jagiello Gruszfeld, Maria Sklodowska Curie National Research Institute of Oncology, Poland
Copyright
©2022 Open Access Journal of Biomedical Science, All rights reserved. No part of this content may be reproduced or transmitted in any form or by any means as per the standard guidelines of fair use. Open Access Journal of Biomedical Science is licensed under a Creative Commons Attribution 4.0 International License
How to cite this article
Agnieszka IJG, Agnieszka M, Pawel K, Dorota N, Anna SOG. Ribocyclib in the Treatment of Recurrent Low Grade Serous Ovarian Cancer: Case Report. 2022- 4(4) OAJBS. ID.000464.
Figure 1: Tumor near the left lumbar muscle (1). In the MR study from 11.01.2021 the greatest dimension of the tumor is 50 mm (A). In the MR from 07.11.2021-40 mm (B).
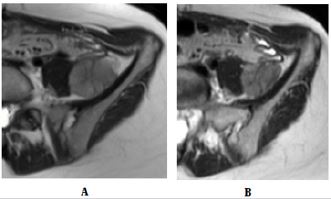
Figure 2: Tumor near the rectal stump (2). In the MR study from 11.01.2021 the greatest dimension of the tumor is 48 mm (A). In the MR from 07.11.2021-39 mm (B).

