Review on Analysis of Breast Tumor with Methods of Treatment
ABSTRACT
Breast malignance is the greatest public in ladies, with a high incidence in North America and Eastern Europe, medium in Southern Europe and the Middle East and low in the Far East. Breast malignance is the second most common malignance in the world after lung malignance, and since it happens a lot, the doctors asked the women to examine themselves by themselves, in order to discover the signs of the disease early before it spreads. It is possible that this disease can be treated after being diagnosed by a specialized doctor and determining the type of tumor in the breast, and the surgeon removes the breast completely and starts chemotherapy about 6 doses, then radiotherapy, how many sessions will be determined by the doctor, and then hormonal therapy, a medicine called Tamoxafin or any medicine determined by the doctor, and it is possible. This disease will not come back again if the eyes follow the instructions and do not tire themselves a lot, and remain calm, because malignance is one of the causes of its increased nervous appearance and you try to stop stimulants such as tea, coffee and chocolate because they increase the chance of injury. Also, stop cigarettes, even if drinks have a percentage A small amount of alcohol in response increases the chance of infection, and also exercise, if we practice it regularly, will benefit greatly and reduce the chances of contracting the disease.
KEYWORDS
Review; Malignance; Chemical malignance; Tumor
INTRODUCTION
The sources of breast malignance are not completely branded, but research is still underway on the following factors: Genetic factors: a gene or genes related to breast malignance in humans, the most important of which is ERBB2, and the proliferation of this oncogene was found in (20%) of breast malignance samples. Hormonal factors: The hormones estrogen and prolactin have a major role in stimulating breast cells to grow. Growth factors: such as TGFa (transformation factors) and IGFs (insulin growth factors) that can be secreted from the tumor cell itself to return and stimulate its growth. Estrogen can also influence distant organs to secrete growth factors that in turn stimulate breast cells to grow. Breast malignance is managed by a multidisciplinary medical team, including medical, radiological and surgical oncologists, and is guided by national and international guidelines and procedures. Factors such as treatment, oncologist, hospital, and stage of your breast malignance determine the cost of breast malignance you’ll need to pay. Staging of breast malignance is the first step in helping doctors regulate the best suitable sequence of behavior. Malignance dramatization arrangement Classification for a tumor, nodes, and metastases is a measure of the animal amount and spread of a malignant growth [1-5].
a. The symbol (T) indicates the primary tumor (the primary)
b. The symbol (n) stands for nearby lymph nodes
c. The symbol (m) indicates a malignant tumor.
Breast Malignance
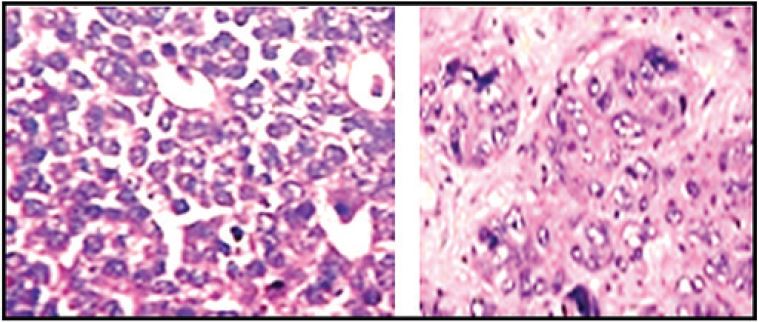
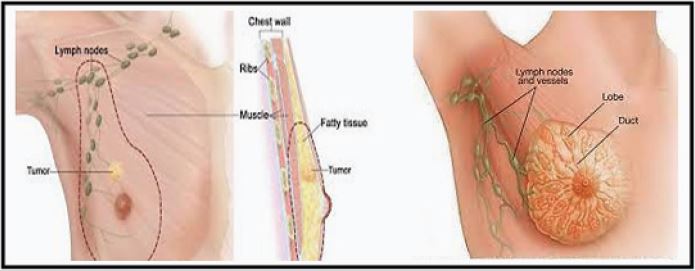
Breast malignance occurs in the breast tissue. The most common type of breast malignance is ductal carcinoma. It begins in the lining of the milk ducts (thin tubes from the breast to the nipple) and there is another type, which is lobular breast malignance and breast malignance is a result of for mutations and changes that are not normal. Tumors may be benign and not dangerous to health, but if they are malignant, they remain dangerous, because benign tumors do not spread and grow slowly, but the malignant spreads outside the original and primary tumor to other parts, and the danger remains that we must remove the ovaries, and this reduces the chances of childbirth and pregnancy after this or the breast Pechal, even if the tumor size is small and not spread, it was replaced by Pechal or in chemotherapy or hormonal treatment.... and with the passage of time the malignance cells enter the breast tissue and make their way to the lymph nodes and burrow under the armpit. In fact, a kind of diagnosis of the disease is that you meet A mass between the armpit and the breast, and this remains a malignant tumor because it can reach the lymph nodes, and after that it begins to spread to other parts of the body [6-10]. Breast malignance is the most common malignance that affects women, and it can also come to men, but at lower rates than women (one man for every 100 women).
Breast Malignance Spread
Significant progress has been made in the treatment of breast malignance since 1980. The age-standardised mortality rate from breast malignance declined by 40% between the 1980s and 2020 in high-income countries. Similar improvement is still to be seen in low- and middle-income countries. Improved outcomes are the result of a combination of early detection and effective treatment using a combination of surgery, radiotherapy, and medical treatments.
Breast Malignance in Women
Before menopause: Changes occur in the breast at different times of the menstrual cycle every month, the milk-producing tissue in the breast becomes effective in the days before the start of the menstrual cycle, and some women feel at this time breast engorgement and hardness, especially near the armpit. After a hysterectomy, the breasts usually continue to show the same natural changes every month until the time when menstruation should stop completely (menopause). After menopause, the activity of the milk-producing tissue stops, and the natural breasts appear tender and less firm than before. In inflammatory occult breast malignance, there may be no symptoms at all. The typical symptoms of breast redness, swelling and inflammation, and sometimes these symptoms may appear during a single night. It is easy to be confused with mastitis [11-15].
Malignance invades the ducts and lymphatic vessels, causing blockage and blocking of drainage, causing the breast to swell. The fluid build-up in the breast may cause it to appear grainy, resembling the shape of an orange peel. Sometimes it is misdiagnosed as an insect bite or a breast infection. In the case of inflammatory breast malignance, there is often no tumor as in the rest of breast malignance s. Although there is a mass in the breast in most cases, in most cases of inflammatory breast malignance it is distributed and without a specific tumor. The tumor may appear suddenly and grow rapidly. Most patients do not have all the symptoms of inflammatory breast malignance. Not all symptoms are necessary to be diagnosed with the disease.
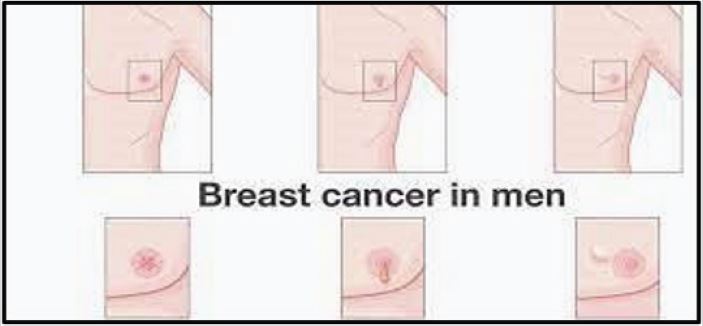
Breast Malignance in Men
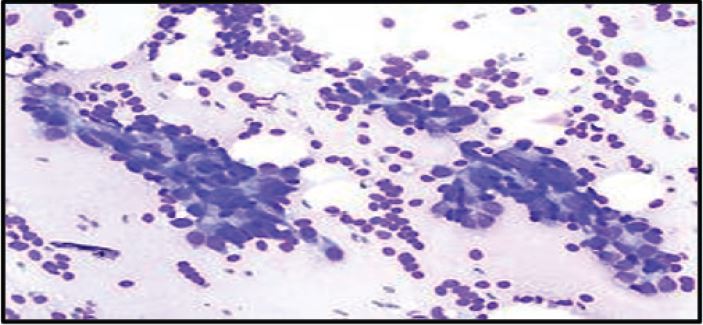
When a man suspects that he has breast malignance, he should go to the doctor for a breast examination. In order to determine if these symptoms are actually caused by malignance, a man may have to undergo another examination or a series of tests to give a definitive diagnosis of the appearance of the disease: Mammography examination, which is known to be effective in women, but less in men. Ultrasound scanning, using an ultrasound scanner that builds a three-dimensional image that helps detect if the mass contains a liquid or a solid. Aspiration is a test in which a needle is inserted into the breast in the area of the lump and a number of cells are suctioned out. This examination is carried out accompanied by an ultrasound image, so that the doctor can be accurate by taking cells from the same lump.
Biopsy, an examination that includes taking a small sample from the cells from the affected area of the breast by a needle The results are sent for examination in a laboratory, they are examined under a microscope to find malignance cells Before the biopsy begins, local anesthesia is administered with an injection Blood tests, to assess general health, Symptoms that should raise questions and concern include a lump in the breast area - which is the main symptom that should raise concern in men , changes in the shape and size of the breast , different secretions from the nipple , wounds in the skin of the breast , a rash around the nipple , The only reliable way to make a diagnosis is to take a breast biopsy. Mammography and ultrasound often show suspicious signs, but often they cannot diagnose the disease. Many conditions, such as mastitis and even heart failure, may mimic the typical symptoms of inflammatory breast malignance.
Fluctuation in symptoms and regression, whether spontaneous or as a result of traditional treatment or hormonal changes, should not be taken into account when diagnosing the disease. It is known that inflammatory breast malignance responds to antibiotics and progesterone, and it cannot be excluded that it may respond to other hormonal and drug treatments [16-25].
Some Infections that cause Breast Malignance
Breast infections may be caused by trauma, engorgement of breast milk, hormonal stimulation, or some autoimmune diseases. Recurrence of infections unrelated to lactation requires endocrinological examination.
Inflammatory breast malignance is classified as a tumor that progresses and infiltrates locally, which means that it has spread to the tissue adjacent to the original source or to nearby lymph nodes. Inflammatory breast malignance is considered an advanced stage of malignance, which means that the tumor has spread far from its point of origin in the adjacent tissue or lymph nodes. Neighbourhood as a possible possibility. It is called inflammatory because it is often associated with symptoms similar to those of inflammation. However, completely different symptoms may appear with him, and in most cases, a tumor is not associated with it, so it is diagnosed by mammography or ultrasound. Only 50% - 75% of cases have typical symptoms, sometimes symptoms are atypical. Inflammatory breast malignance accounts for a small percentage of breast malignance cases (1-6% in the United States) and is most often diagnosed in young women, although the average age of onset is not significantly different from that of other breast malignance cases (average age of 57). year). Recent advances in medicine and treatment have greatly improved diagnostic methods. At least one third of women will survive ten years or more after being diagnosed with the disease.
Breast Malignance Grading
The grading of breast malignance is divided into categories according to the criteria of different systems, and for different purposes. The main categories are tissue type, tumor grade, tumor stage and expression of proteins and genes. These classifications are updated as the biology of malignance cells develops.
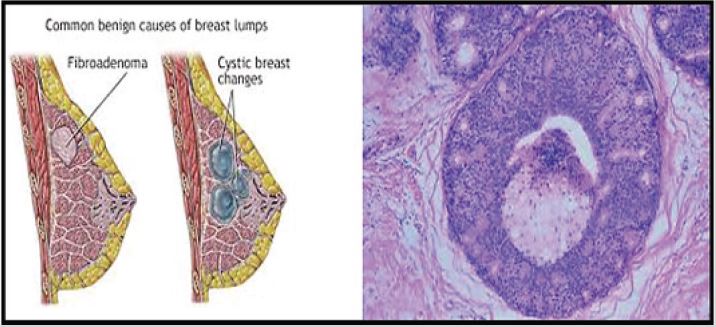
Breast Fibroids
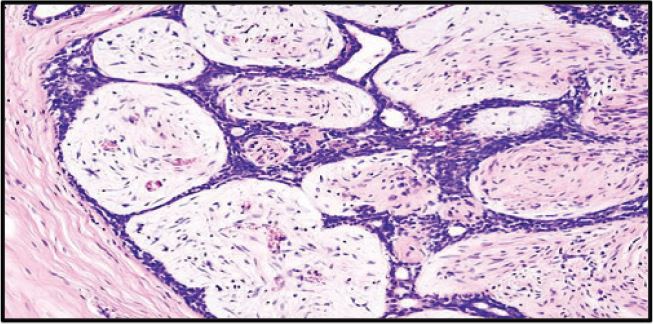
The breast consists of milk-secreting glands and milk ducts surrounded by fibrous tissue, glandular tissue, and fatty tissue. A fibroadenoma is a non-malignance mass that arises from glandular and fibrous tissue with no known cause. Fibroid tumor is the most common breast tumor in women under the age of 30. The symptoms of fibroadenoma are similar to those of breast malignance in that a strange lump appears in the breast and the difference is in the mobility of the fibroadenoma while the breast malignance lump is stable and immobile. A fibroadenoma requires medical follow-up to ensure that it develops in size over time, and the patient may need surgery to remove it. Fibroid tumors may be called mouse breasts or mice breasts due to the mobility of the fibroadenoma within the breast tissue. 10-15% of patients with fibroadenoma have multiple lumps in both breasts, while the majority of patients have only one lump. The fibroadenoma lump is elastic, painless, easily movable, with easily distinguishable sides and a smooth surface. The size of the fibroadenoma varies from a few millimetres whose presence cannot be identified until using a mammogram or ultrasound, to a few centimetres that can be felt by medical examination, to huge sizes of up to 8cm. The fibroadenoma may increase in size over time, especially in Pregnancy, and may atrophy during the menopause in the patient [26-30].
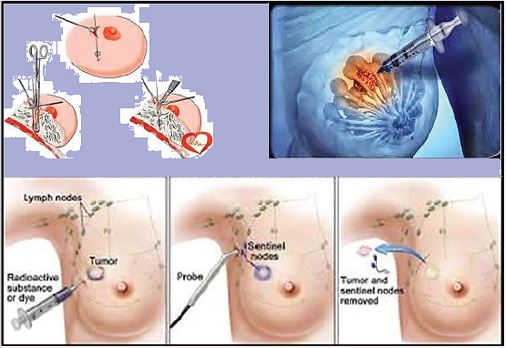
METHODS OF TREATMENT
Treatment includes chemotherapy with a combination of other treatments, radiotherapy, hormonal therapy when needed and in some cases surgery. Estrogen inhibitors or hormonal inhibitors show positive improvement. Surgery was done infrequently because inflammatory breast malignance is systemic malignance, however surgery may improve the final outcome and is now being considered. Resection of only part of the breast is not an option in patients with inflammatory breast malignance. Resection of the lymph nodes is also recommended. Swelling of the arm and hand on the side where the surgery was performed, may be a complication of lymphadenectomy. Breast reconstruction is an option for patients who have had a mastectomy after their recovery. In the case of smokers and women with diabetes, complications are more common.
Radiation Therapy
Diagnosis of fibroadenoma requires a medical examination by a specialist in addition to mammography or ultrasound in younger patients, and in the case of suspicious tumors, the doctor may resort to a breast biopsy to reach the correct diagnosis. Breast malignance is the supreme mutual malignance in the Kingdom, and among ladies. Breast malignance in the Kingdom is more common among women aged 40 years and over. More than 50% of breast malignance cases in the Kingdom are detected in advanced stages, compared to 20% in developed countries [31-42].
This increases the mortality rate and reduces the chances of recovery, as well as the high cost of treatment. The early detection of breast malignance by mammography, greatly increases - by the grace of God - the rate of cure and survival and increases treatment options and efficacy. The total number of malignance cases in the Kingdom, according to the latest statistics of the Saudi Malignance Registry in 2016, reached (16,859), of which (13,161) were among Saudis, with a percentage of 78.1%, of which 44.1% were males, while 55.9% were women. Breast malignance ranked first (2282 cases), at 17.3% of both sexes, and 30.4% of all malignance s in women.
Then followed by colorectal malignance, then thyroid malignance, with an infection rate of 27.2 per 1,000 Saudi women. The eastern region ranked first in the number of infections with a rate of 46.7/1000, followed by Riyadh with a rate of 33.8/1000, then Al-Qassim region with a rate of 31.7/1000, Makkah Al-Mukarramah with a rate of 29.7/1000, and Al-Jawf ranked fifth with a rate of 25/1000. The median age of injury was 50 years (Figure 1-7).
CONCLUSION
Unfortunately, even if all modifiable risk factors could be controlled, this would reduce the risk of breast malignance by only a maximum of 30%. Gender (female) is the strongest risk factor for developing breast malignance, with the incidence of breast malignance in men not exceeding 0.5-1%. Breast malignance treatment for men follows the same principles as for women. The risk of developing a family history of breast malignance is increased.
REFERENCES
- Seattle (WA) (2020) Institute for Health Metrics, University of Washington, USA.
- Ferlay J, Ervik M, Lam F, Colombet M, Mery L, et al. (2020) Global malignance observatory: Malignance today. International Agency for Research on Malignance, Lyon, France.
- Weber DJ, Rutala WA (2013) Self-disinfecting surfaces: Review of current methodologies and future prospects. American Journal of Infection Control 41(5): S31-S35.
- Nagham MA, Aseel MJ, Imd K (2020) Public Health in Hospitals (1st edn). Eliva Press, Moldova, ISBN: 9798636352129.
- Martel DC, Georges D, Bray F, Ferlay J, Clifford GM (2020) Global burden of malignance attributable to infections in 2018: a worldwide incidence analysis. The Lancet Global Health 8(2): e180-e190.
- Jawad AM, Nagham MA, Jwad SM (2020) Development and preparation of ciprofloxacin drug derivatives for treatment of microbial contamination in hospitals and environment. Indian Journal of Forensic Medicine & Toxicology 14(2): 1115-1122.
- Imd K, Hasnen KA, Nagham MA (2020) Invention of (Gluta.Sulfazane- Cefixime) compounds as inhibitors of malignance Tumors. Journal of Cardiovascular Disease Research 11(2): 44-55.
- Haas JS, Kaplan CP, Brawarsky P, Kerlikowske K (2005) Evaluation and outcomes of women with a breast lump and a normal mammogram result. Journal of General Internal Medicine 20(8): 692-696.
- Nagham MA, Hsein MA (2021) Synthesis and characterization of some new formazan - cefixime and study of against breast malignance cells. Annals of the Romanian Society for Cell Biology 25(4): 8562–8578.
- Nagham MA, Asmaa KM (2021) Synthesis, identification and antimalignance studying of heterocyclic- mefenamic drug via thiosemicarbazide. Annals of the Romanian Society for Cell Biology 25(4): 8521-8537.
- Eischeid AC, Linden KG (2011) Molecular indications of protein damage in adenoviruses after UV disinfection. Applied and Environmental Microbiology 77(3): 1145-1147.
- Thomadsen B, Ravinder N, Bateman FB, Jonathan F, Glisson C, et al. (2014) Potential hazard due to induced radioactivity secondary to radiotherapy. Health Physics 107(5): 442-460.
- Nagham MA (2017) Synthesis of antifungal chemical compounds from fluconazole with (Pharma-Chemical) studying. Research Journal of Pharmaceutical, Biological and Chemical Sciences 8(3): 564 -573.
- Abdullabass HK, Jawad AM, Nagham MA (2020) Synthesis of drugs derivatives as inhibitors of malignance ous cells. Biochem Cell Arch 20(2).
- Nagham MA, Imd K (2020) Development of trimethoprim drug and innovation of sulfazane-trimethoprim derivatives as antimalignance agents. Biomedical and Pharmacology Journal 13(2): 613-625.
- Mahdi AK, Nagham MA (2020) Heterocyclic derivatives with aspirin drug (synthesis, characterization, studying of its effect on malignance cells). International Journal of Cell Biology and Cellular Processes 6(2): 30-37.
- Wild CP, Weiderpass E, Stewart BW (2020) World malignance report: Malignance research for malignance prevention. International Agency for Research on Malignance, Lyon, France.
- Jawad F, Nagham MA (2021) Preparation, investigation, and study of biological applications of tyrosine derivatives against breast malignance cells. NeuroQuantology 19(9): 117-125.
- Haverstick S, Goodrich C, Freeman R, James S, Kullar R, et al. (2017) Patients’ hand washing and reducing hospital-acquired infection. Critical Care Nurse 37(3): e1-e8.
- Molins RA (Ed.) (2001) Food irradiation: principles and applications. John Wiley & Sons, USA.
- Nagham MA, Jawad F (2021) Preparation, diagnosis and evaluation of cyclic-tryptophan derivatives as anti-breast malignance agents. Biomedical and Pharmacology Journal 14(4).
- Nagham MA (2022) Designation of macrocyclic Sulfazan and Triazan as innovated compounds with their estimation in nano-activities by the scanning microscope. International Journal of Convergence in Healthcare 2(1): 25-34.
- Diehl JF (2002) Food irradiation - past, present and future. Radiation Physics and Chemistry 63: 211-215.
- Rutala WA, Weber DJ (2008) Guideline for disinfection and sterilization in healthcare facilities, CDC.
- Rutala WA, Weber DJ (2010) Guideline for disinfection and sterilization of prion-contaminated medical instruments. Infection Control Hospital Epidemiology 31(2): 107-117.
- Hsein MA, Nagham MA (2021) Synthesis and characterization of new trimethoprim-formazan derivatives with studying them against breast malignance cells. International Journal of Biochemistry and Biomolecules 7(1).
- Roth S, Feichtinger J, Hertel C (2010) Characterization of Bacillus subtilis spore inactivation in low-pressure, low-temperature gas plasma sterilization processes. Journal of Applied Microbiology 108(2): 521– 531.
- Nagham MA (2021) Inventing of macrocyclic formazan compounds and studying them against breast malignance for the first time globally. Annals of Pharma Research 9(7): 525-533.
- Nagham MA (2021) Creation of innovated macrocyclic sulfazanformazan compounds and linear sulfazan-formazan for the first time globally with their assay as antifungal. Biomedical Journal of Scientific & Technical Research 40(3): 32266-32272.
- Kanemitsu K, Imasaka T, Ishikawa S, Kunishima H, Harigae H, et al. (2005) A comparative study of ethylene oxide gas, hydrogen peroxide gas plasma, and low-temperature steam formaldehyde sterilization. Infection Control Hospital Epidemiology 26(5): 486-489.
- Mushtaq M, Banks C J, Heaven S (2012) Effectiveness of pressurised carbon dioxide for inactivation of escherichia coli isolated from sewage sludge. Water Science and Technology 65(10): 1759-1764.
- McDonnell G, Burke P (2003) The challenge of prion decontamination. Clinical Infectious Diseases, 36(9): 1152-1154.
- Nagham MA (2016) The challenge of prion decontamination. Clinical infectious diseases. Der Pharma Chemica 8(6): 40-48.
- Irshad A, Ackerman SJ, Pope TL, Moses CK, Rumboldt T, et al. (2008) Rare breast lesions: Correlation of imaging and histologic features with WHO classification1. Radiographics 28(5): 1399-1414.
- Nagham MA (2015) Synthesis and chemical identification of macro compounds of (thiazol and imidazol). Research Journal of Pharmacy and Technology 8(1): 78-84.
- Rogez KC, Yousfi R, Soufflet C, Quadrio I, Yan ZX, et al. (2009) Inactivation of animal and human prions by hydrogen peroxide gas plasma sterilization. Infection Control Hospital Epidemiology 30(8): 769-777.
- Shireen RR, Nagham MA, Ali Jassim AZ (2020) Guanine substituted heterocyclic derivatives as bioactive compounds. Biochemical and Cellular Archives 20(2): 3651-3655.
- Bauman PA, Lawrence LA, Biesert L, Dichtelmüller H, Fabbrizzi F, et al. (2006) Critical factors influencing prion inactivation by sodium hydroxide. Vox sanguinis 91(1): 34-40.
- Jolesz FA, Hynynen K, McDannold N, Tempany C (2005) MR imagingcontrolled focused ultrasound ablation: A noninvasive image-guided surgery. Magnetic Resonance Imaging Clinics of North America 13(3): 545-560.
- Gombos EC, Kacher DF, Furusawa H, Namba K (2006) Breast focused ultrasound surgery with magnetic resonance guidance. Topics in Magnetic Resonance Imaging 17(3): 181-188.
- Hynynen K, Pomeroy O, Smith DN, Huber PE, McDannold NJ, et al. (2001) MR imaging-guided focused ultrasound surgery of fibroadenomas in the breast: A feasibility study. Radiology 219(1): 176-185.
- Marret H, Bleuzen A, Guérin A, Herbreteau D, Patat F, et al. (2011) Résultats préliminaires de la destruction des fibromes utérins par ultrasons focalisés contrôlée par résonance magnétique. Gynécologie Obstétrique & Fertilite 39(1): 12-20.
Article Type
Research Article
Publication history
Received Date: January 25, 2022
Published: February 18, 2022
Address for correspondence
Nagham Mahmood Aljamali, Department of Chemistry, Synthetic Organic Chemistry, Iraq
Copyright
©2022 Open Access Journal of Biomedical Science, All rights reserved. No part of this content may be reproduced or transmitted in any form or by any means as per the standard guidelines of fair use. Open Access Journal of Biomedical Science is licensed under a Creative Commons Attribution 4.0 International License
How to cite this article
Nagham MA, Aliaa HM, Maryam JN. Review on Analysis of Breast Tumor with Methods of Treatment. 2022- 4(1) OAJBS.ID.000400.