Respiratory Physiology in Swimming and Diving: A Review
ABSTRACT
The respiratory system including airways, lungs and blood vessels is the setup of organs and tissues that help the human breathe. The lungs are the central organ of the respiratory system, involving in the exchange of respiratory gases to provide oxygen to various tissues in the body and remove carbon dioxide (CO2). Continuous consideration and monitoring of respiration and circulation provide immense information for biomedical engineers to understand the variables of the respiratory and circulatory systems that show how well these systems work. From the physiological perspective, respiration and circulation are two body processes that are most affected during swimming and diving. This review paper aims to briefly explore the effect of swimming and diving on the respiration physiology comprising respiratory muscles. The human respiratory system and its importance in human life are well documented. The biomechanics and physiology of swimming and diving and also current understanding of the physiological changes in the human respiratory system are demonstrated. The information given in this paper can be used as an important guide to minimise the health risks associated with recreational water activities.
KEYWORDS
Respiratory system; Lungs; Biomedical; Gas exchange; Muscle fatigue
INTRODUCTION
Swimming is one of the most popular aquatic sports worldwide and diving is one of the most exciting and challenging sports in the world. However, some researchers have reported the injuries of swimming and diving on the human body, especially on the respiratory system. Some common swimming injuries include inspiratory muscle fatigue Lomax [1]; Thomaidis et al. [2]; Brown [3]; Lomax et al. [4]; Lomax et al. [5], shoulder injury Rupp et al. [6]; Sein et al. [7], hip adductor injury Grote et al. [8], breaststroker’s knee Stulberg et al. [9], lumbar intervertebral disk degeneration Kaneoka et al. [10], musculoskeletal injuries Gaunt [11] and low oxygen uptake by swimmers due to respiratory limitations, central circulatory, peripheral/muscular capacities for oxygen transport and use Holmer [12]. Besides, injuries related to diving should not be ignored. Lindholm [13] states that during diving, the respiratory system is injured by problems such as compression of the lungs with barotrauma of descent, intrapulmonary hemorrhage, edema, and the effects of glossopharyngeal insufflation and exsufflation. Moreover, Lane 1988 explains that although the human ability while diving underwater is extremely limited physiologically, insight into such limitations increases safety of diving.
Literature review shows that despite several review papers related to cardiovascular responses and renal effects of aquatic exercise Epstein [14,15], non-submersion injuries associated with aquatic sporting and recreational activities including swimming, fishing and boating Chalmers [16], the ventilatory responses to immersion and changes in water temperature Datta [17], the physiology and pathophysiology of human breath-hold diving Lindholm [13], physiological aspects of swimming and diving while breathing at depth Tetzlaff [18]; Bosco et al. [19] the physiological necessities of artistic swimming, the physiological characteristics that affect the performance of this type of swimming, and innovative strategies for increasing training and performance in elite individuals Viana et al. [20], applying smart wearable devices to improve safety and performance in breath-hold diving Vinetti et al. [21] and the physiology of deep diving Patrician et al. [22], factors affecting the change in lung function in athletic swimmers Rochat et al. [23], the physiology of human respiratory system during swimming and diving have not been completely addressed.
Several research have been conducted during the last two decades to better understand the biomechanics and physiology of swimming. Findings from past research studies and information reviewed in this paper about recent progress and advances of physiological changes in the human respiratory system during swimming and diving can be effectively used as key guidelines for swimmers and coaches in their efforts to develop the capacities of their experts and explore the limits of human performance. Hence, this article deals with the physiological changes, the biomechanics as well as the main injuries of the human respiratory system in aquatic environments during swimming and diving. First of all, the paper will focus on human respiratory system, examine its significance in human life and evaluate the secondary functions of this system. Secondly, this paper will identify the main injuries in the literature associated with swimming and diving. Eventually, this review paper will use authors’ personal opinions and ideas about the respiratory physiology in swimming and diving to explore a possible response. This review can be used as an important guide to minimize the risks of swimming and diving.
To recognize the literature for this review we undertook PubMed as an interface and a search engine for a systematic search of Medline database of references on biomedical topics. We also identified the relevant articles by examining the reference lists found at the end of published research papers, review articles and books. We also employed Google Scholar web search engine to discover scientific literature related to biomechanics of lungs. The following keywords and terms were used for database search: Human respiratory system, respiratory physiology, swimming, diving, gas exchange, injuries, respiration and circulation, respiratory muscles, biomechanics of lungs, physiology of swimming and diving, physiological changes, muscle fatigue, depth of diving, breath-hold time, apnoea trainings and aquatic environments. These searches were generally restricted to English-language publications. Because of the disparate nature of the literature, this current review is subdivided into sections specifically addressing human respiratory system and its physiological changes, factors affecting the performance of swimming and diving and related respiratory problems.
HUMAN RESPIRATORY SYSTEM
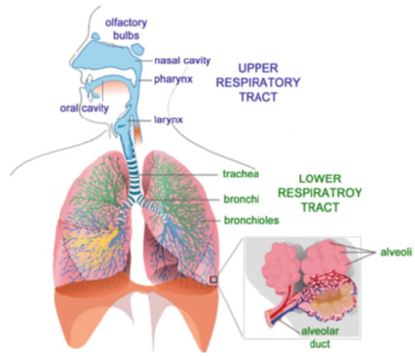
Gas exchange in the human respiratory system plays an important role in human life. The function of the respiratory system is based on this process, in which oxygen is taken from the atmosphere and carbon dioxide is removed from the blood NOAA Diving Manual [24]. It is important to note that oxygen is essential for normal metabolism and carbon dioxide is a waste product of this metabolism. Carbon dioxide is only inhaled in small amount this gas is produced in the body metabolism by decarboxylation processes as a reaction product and subsequently exhaled. Tu et al. [25] provided a detailed description of the human respiratory system. In the human body, there are millions of alveoli in the lungs where the exchange of oxygen and carbon dioxide occurs. During gas exchange oxygen moves from the lungs to the bloodstream. Simultaneously, carbon dioxide is transported in the blood from body tissues and back to the lungs. This phenomenon occurs when oxygen first enters the nose or mouth while breathing. Air passes through the larynx and trachea and then divides into two bronchi. Each bronchus splits into two smaller branches and forms the bronchial tubes. These tubes form many pathways inside the lungs and eventually connect to tiny sacs called alveoli. The exchange of gases takes place in the alveoli, where oxygen diffuses into the capillaries of the lungs to exchange with carbon dioxide. After the exchange of gases, the air comprising carbon dioxide begins to return through the bronchial paths and returns to the external environment through the nose or mouth. Secondary functions of the respiratory system include filtering, warming, and humidifying the inhaled air. In this regard, the vocal cords of the larynx produce sound, the lungs control the body’s pH level, and the olfactory bulbs in the nose cause smelling. Figure 1 schematically shows the human respiratory system including the upper and lower respiratory tract regions.
PHYSIOLOGICAL CHANGES IN THE HUMAN RESPIRATORY SYSTEM
Swimming and diving cause physiological changes in the human respiratory system. Several research have been conducted during the last two decades to better understand the biomechanics and physiology of swimming. The results have become as guidelines for swimmers and coaches in their efforts to develop the capacities of their adepts and explore the limits of human performance. The research works presented by Holmer [12], Cordain [26]; Wylegala et al. [27]; Lomax et al. [4]; Ferreira et al. [28] are all noteworthy. Holmer [12] explains that swimming takes place in water environment, that presents completely different gravitational and resistive forces compared to air. The swimmers are in a horizontal position which alters gravitational effects on the circulation system and respiratory physiology. Breathing is limited by swimming stroke mechanics and the water environment. Given these conditions, thermoregulatory demands are not balanced with metabolic demands during heavy exercise in a water environment with its own thermodynamic properties. Lin [29] highlights that exercise during intense swimming severely changes the thermoregulation in the water environment. If the water temperature is low enough and the insulation is inadequate, even if the heat production is 10 to 15 times higher than the basal temperature, the body temperature may drop. Pendergast et al. [30] explain that water properties define the mechanical load and the physiological responses during swimming in water. Blood translocation into the thorax and elevation of plasma volume results in increased cardiac stroke volume and output and affects pulmonary blood flow and gas chambers. Immersion results in an increase in ventilation. An increase in the blood volume in the lungs leads to capillaries obstruction, which displaces gas volume and may increase the risk of pulmonary edema. Bosco et al. [19] described the physiological changes caused by immersion, swimming, and diving. They also demonstrated cardiac, circulatory and pulmonary vascular adaptation, and the pathophysiology of new syndromes that allow the swimmers and divers to succeed in a variety of environments.
Water Resistance
The relationship between water resistance and propulsion in swimming have been analysed in recent decades. Several researchers investigated the dependence of water resistance against swimmers’ propulsive force on body size, body crosssectional area, body form, and body position in water Clarys [31]. It was found that at a certain speed, female swimmers showed less resistance than the men. The reasons for this can be attributed to their body form and smaller body size, which cause a higher horizontal position in the water. Clarys [32] further investigated the ergonomics links between fundamental hydrodynamics, applied dynamics of swimming, electromyographical (EMG) features and special training. The passive drag in different positions and active swimming drag were measured. The researcher found that drag in a prone position under the water surface was greater than at the water surface. Moreover, active drag while swimming reached twice the drag values of any passive drag condition. This indicates that body form has no effect on drag and propulsion. However, further researchers found little or even no difference between the active and passive drag values Toussaint et al. [33].
Factors Affecting Swimming Performance
A combination of a number of factors may be effective in improving swimming performance. Holmer [12] demonstrated that a successful performance in swimming is the result of a complex interaction of several factors including physical, biomechanical, physiological and psychological factors. Holmer [12] quoted this claim that swimming with controlled frequency breathing can improve the anaerobic power. This type of respiration prevents the production of metabolic acidosis by swimmers and causes the production of respiratory alkalosis. In order to maintain the normal acid-base balance, it is necessary that all acids produced be equal to all the excreted acids Seifter [34]. Respiratory alkalosis can be caused by hyperventilation and is characterised by a low arterial blood PCO2 and high pH value due to low H+ ion concentration Kamel [35]. However, respiratory acidosis is the acid-base interference results by an increase in PCO2 of blood Vepraskas et al. [36]. Respiratory acidosis often takes place as a consequence of acute pulmonary disease or weakness of respiratory muscle and chest wall or unusual gas exchange through the pulmonary capillary Hamm [37]. In a study, Lemaitre et al. [38] examined the effect of extra respiratory muscle endurance training (RMET) on the respiratory muscle function and swimming performance of young well-trained swimmers. The researchers divided the swimmers into two groups: group RMET and group non-RMET. The duration of RMET was considered to be eight weeks. All athletes in both groups followed similar training sessions, 5 to 6 times a week. They assessed the strength and endurance of the swimmers’ respiratory muscles, their performance in the 50- and 200-meter trials, and perception of effort and Shortness of breath (dyspnea) before and after the investigation. The results revealed that the extra respiratory muscle endurance training was able to improve the parameters of ventilation function, chest expansion, respiratory muscle strength and endurance, as well as swimming performances in group RMET. Rochat et al. [23] reviewed the important factors that influence the change in lung function in athletic swimmers. They found that swimmer athletes had better expiratory flow, higher baseline lung volumes and better pulmonary function compared to non-athletes and untrained individuals. The authors further explained that most of these characteristics can be due to changes in lung growth as a result of intensive training over time. However, the contribution of genetic factors cannot be ignored.
Effect of Water Pressure
Due to the fact that diving is done in an environment with a pressure higher than the normal atmospheric pressure, it may have a significant impact on the human respiratory system. Lin [29] clarifies that diving is related to exposure to the pressure which is greater than the atmospheric pressure. Diving is divided into two types: breath-hold diving and Scuba diving in which the diver uses a self-contained underwater breathing apparatus. Breath-hold diving can offer divers freedom and mobility. Exposure to factors related to high pressure and gas mixture, such as hyperoxia, decompression stress, and gas density, has severe effects on pulmonary function that may limit ventilation capacity and exercise tolerance. The effects of hyperoxia and decompression stress are very harmful, which can result in serious inflammatory reactions and long-term illness. Lin 1988 examined diving accidents separately according to the type of diving. The author stressed that the accidents related to scuba diving are complex. These accidents include problems with equipment, inert gas narcosis, oxygen toxicity and the most importantly, decompression diseases. In contrast, accidents associated with breath-hold diving are often physiological and generally involve drowning. In addition, the environment in which diving takes place may place more physiological constraints on the performance of divers Etzlaff [18]. Mijacika [39] highlight the extreme environmental factors such as increased hydrostatic pressure, hypoxia, hypercapnia, hypothermia and drastic exercise on breath-hold diving, which make this type of diving a threat to the diver in the water environment. According to these authors, severe lungs injury in breath-hold diving includes pulmonary barotrauma, noncardiogenic pulmonary oedema or haemoptysis.
Breath-Hold Time and the Depth of Diving
In breath-hold diving, determining the breath-hold time (BHT) and the depth of diving can lead to a successful and healthy diving. According to Lin [29], calculation of the breath-hold time (BHT) in breath-hold diving is very important as it may prevent physiological accidents for divers. BHT can be obtained from the following oxygen supply-demand relationships (quoted in Lin [29]):
Assuming that the gas is oxygen, the breath-hold time can be expressed as follows:
BHT=VC/VO2 (STPD)×(Pb-47)/863
If air is used to calculate the breath-hold time instead of oxygen:
BHT=TLC × FAO2/VO2 ×(Pb-47)/863
where,
BHT represents the breath-hold time (min), VC and TLC denote the vital capacity and total lung capacity (mL) at body temperature (37 °C or 310 K) and pressure (same as ambient pressure), respectively, VO2 stands for the oxygen consumption (mL/min) at standard temperature (0 °C or 273 K) and pressure (760 mmHg or 101.33 kPa), dry (no humidity) (STPD), FAO2 is the alveolar fraction of oxygen and Pb -47 is referred to the barometric pressure (torr, 1 torr equals 133.322 pascals).
Another important parameter in breath-hold diving is diving depth, which must be determined, accurately. Short diving time is certainly one of the factors that prevent divers to reach deeper zones of water. The diving depth for humans is estimated to be equal to the ratio of the total lung capacity to the residual volume in terms of atmosphere, and is obtained from the following equation Lin [29]:
D= Pb ×(TLC/RV-1)×10
where,
D is the diving depth (m), Pb signifies the barometric pressure (atm), TLC represents the total lung capacity (mL), RV denotes the residual volume (mL) and 10 is referred to the depth in terms of metres equivalent sea water of 1 atmosphere.
Diving Limitations
A number of authors have highlighted the limitations of diving. One of the imperative limitations of divers in aquatic environment is that hypothermia certainly occurs following long-term water immersion. The thermo-neutral temperature for the human body in the aquatic environment is 35 degrees Celsius Pendergast et al. [30] at which the human body neither loses nor receives heat. This temperature is much higher than ocean water. Thermal flow continues as long as the diver is in the water, resulting in hypothermia. Hypothermia can affect the functioning of all organ systems. Cardiac disorders, irregular thinking, sensory and motor injury, loss of consciousness and drowning are all the result of hypothermia and occurs when the body temperature falls below 35 °C. Appropriate insulation is the only protection for the diver against hypothermia. Besides, as soon as the body temperature drops below the thermo-neutral temperature, the diver must stop diving and resume it after the body organs have warmed up Lin [29]. However, heat may also be supplied by external supplementary systems such as battery-powered heater-pump systems Rawlins [40]. Diving in thermo-neutral water causes significant physiological changes that are even more complex than cold water. The physiological effects of immersion in water include respiration, blood circulation, regulation of body fluids and regulation of temperature. Headout water immersion causes blood to shift toward the upper body, which in turn increases central blood volume Epstein [15], which results in obstruction of the vasculatures in the thoracic region Lin [29]. There are some reasons for increase of the central blood volume including hydrostatic compression which reduces vein capacity in the lower limits displacing abdominal contents toward the chest and a negative transthoracic pressure which also promotes redistribution of circulating blood toward the upper body. The heart rate changes slightly during immersion in thermo-neutral water. Cold water lowers the heart rate. However, an increase in metabolic demands during diving increases it. This is only true as long as body temperature does not fall. As the water temperature falls, the heart rate also decreases, leading to a slight increase or even decrease in cardiac output Lin [29]. Castellini et al. [41] presented an inverse relationship between diving duration and metabolic rate. Cardiac output increases by the same rate as stroke volume in thermo-neutral water Lin [29]. Pendergast et al. [30] reported that lowering the water temperature in water immersion conditions does not affect the cardiac output compared to thermoneutral temperature. However, the heart rate and the distribution of muscle and fat blood flow may be affected. Investigation conducted by Datta [17] discovered that immersion in cold water results in slower respiration, which is more intense than the decreased metabolic demand realized with hypothermia, resulting in hypercapnia and hypoxia. Some researchers have noted the diuretic effect of immersion in water. As the urine output increases, the plasma volume decreases. Secondary effects, such as decreased work capacity, orthostatic intolerance, and other circulatory function disorders will occur. Dehydration during a long stay in water, even at thermo-neutral temperature is a major problem Epstein [14]. Epstein [15] reported a considerable diuresis during immersion in water. Diuresis after water immersion is caused by neurohumoral factors. Long-term immersion in water changes neurohumoral regulation of kidney function Pendergast et al. [30]. When humans are immersed in cold water, cold temperatures and hydrostatic pressures stimulate significant diuresis. The diuretic response of divers may be due to the cooperative stimulation of the Henry-Gauer reflex when cold stress is superimposed on immersion stress. Hydrostatic compression of the skin is essential for creating natriuresis when immersed in cold water. Immersion in water greatly reduces vital capacity and increased sodium excretion. Increased urinary Na / K values show preferential excretion of sodium ions by the rental tubule during immersion in thermoneutral and cold-water Knight [42]. Greenleaf et al. [43] explained that the Gauer-Henry reflex is not the main mechanism of diuresis due to immersion. Other diuretics are also involved.
Effect of Diving on the Human Respiratory System
Some researchers have studied the effect of diving on the human respiratory system. According to Lin [29], the effect of diving on the respiratory system can be examined on three imperative issues: (1) Immersion in water reduces lung volume by about 5 to 10%, mainly due to a decrease in expiratory reserve volume. Factors such as blood pooling and displacement of the diaphragm toward the chest play an important role in reducing lung volume during immersion. (2) An increase in the central blood volume during immersion tightens lung tissues, which reduces lung adaptation, compresses small airways, increases airway resistance and elevates air trapping and closing volume. The combination of these changes rises the load on the respiratory muscles. (3) Immersion in water due to opposing factors has no effect on gas exchange at rest or during exercise. It is possible to increase gas exchange during immersion in water due to the increase in central blood volume and the removal of dependence of blood flow on gravity, which promotes homogeneous perfusion of the lungs. According to Lin [29], although the same mechanism does not function for the distribution of gas within the lungs, a decrease in alveolar ventilation to an irregular distribution of blood flow was prominent. This advantage is balance by an increase in intrapulmonary shunt, trapped gas, closing volume, and lung stiffness. Choukroun [44] investigated the respiratory gas exchange in human during immersion in water at different temperatures. In this study, three different temperatures selected including 34 °C (thermo-neutral water), 25 °C (cold water) and 40 °C (hot water). They employed a rebreathing method using the inert gas Freon 22 to measure cardiac output and pulmonary tissue volume. Furthermore, the authors determined the oxygen consumption by the closed-circuit procedure. Besides, a micro-method and a mass spectrometer were utilized to analyze arterial blood gases (PaO2, PaCO2) and alveolar gas (PAO2) during quiet breathing, respectively. They found that the immersion into cold water 25 °C had no substantial effect on cardiac output. However, immersion in a hot water (40 °C) resulted in a significant increase in cardiac output. The results further revealed that immersion in water at any of the temperatures had no effect on pulmonary tissue volume. Also, a significant increase in metabolic oxygen consumption was only detected at 25 °C. Moreover, arterial blood gases were slightly affected by immersion in water at the above temperature range. Further investigations conducted by Choukroun [44] exposed those two major factors including hydrostatic pressure and temperature can affect oxygen transport during immersion. Above the neutral temperature, oxygen transport was improved due to a significant increase in cardiac output because of a combination of hydrostatic counter pressure and body heating. Below the neutral temperature, the transport process was changed.
In a study, Clark [45] measured oxygen effects on pulmonary function in men who breathed oxygen continuously at pressures varying between 3.0 and 1.5 atmospheres for average intervals of 3.4, 5.7, 9.0, and 17.7 hours, respectively. The rates of development of effects of pulmonary oxygen toxicity were monitored. The results found that continuous oxygen exposure at above mentioned pressure range affects pulmonary mechanical function prior and more obviously than carbon monoxide diffusing capacity. By defining inherent limits of oxygen tolerance in man, the author provided appropriate guidelines for safe and efficient applications of hyperoxia in diving operation.
Effect of Physical and Apnoea Trainings
Some researchers have studied the effect of physical and apnoea trainings on the apnoeic period and consequently on diving performance. According to Schagatay et al. [46], physical training and apnoea training can be the components of active diving that increase the apnoeic period. They investigated the effects of two types of training including physical and apnoea training on the diving reaction and apnoeic period in humans. They also examined the influences of both training groups on the characteristics of the rise in apnoeic period with frequent apnoea. The results found that an increase in apnoeic period was detected after physical training, and this was related to an increased time beyond the physiological breaking point. The results further show that after apnoea training, apnoeic period was increased by a delay in the physiological breaking point, which is mostly determined by the arterial tension of dioxide carbon.
These researchers further state that frequent performance of apnoea may be the principal cause in delaying the physiological breaking point and promoting bradycardia. The results obtained by these researchers can clarify the prominent diving responses and long apnoea detected in trained apnoeic divers. In a study, Andersson et al. [47] revealed that during apnea, the heart rate and arterial oxygen saturation decreased, and blood pressure increased. Lin et al. [48] explains the physiology of breath-hold breaking point. They state that the course of breath-hold can be specified by voluntary inhibition of respiratory muscular activity, onset and retained involuntary ventilator activity with glottis closed and voluntary opening of glottis. However, glottis opening, and closing is difficult to control directly for most people Massery et al. [49]; Du Toit [50].
Respiratory Problems
Respiration and circulation are two body processes that are most affected during diving. Etzlaff [16] introduced diving techniques, physics and the associated human physiology, and pathophysiology related to the underwater environment. They described the causes of major medical problems that may occur in diving with an emphasis on the basic respiratory physiology. They concluded that appropriate physiologic function and respiratory system adaptation are important to minimize the dangers associated with diving. Etzlaff [18] highlighted that during diving, divers are exposed to hazards that are unique to the highpressure underwater environment and the physical behavior of the gases at higher ambient pressures. Hypercapnia, hyperoxia, carbon monoxide poisoning, inert gas (mostly nitrogen) narcosis, and decompression sickness can all lead to loss of consciousness. In these non-respiratory conditions, the risk of drowning is high. These kinds of diving problems are what respiratory system specialists such as Lindholm [13] have highlighted the major challenges of breath-hold diving including duration and its connection with hypoxia, depth which causes mechanical strain on air-containing body cavities by compression and the exposure to high gas pressures with potential pharmacological/toxic effects.
The literature review shows that swimming and diving affect the physiology of the body’s respiratory system and may cause problems for human health. The main reason of respiratory problems is the lack of proper access of tissues to oxygen or improper elimination of carbon dioxide from tissue cells. Respiratory muscle fatigue is an important physiological problem of diving on humans, which their strength, power and endurance can be increased using special trainings. In addition, the stimulation of the respiratory muscles can also cause physiological changes in their function.
CONCLUSION AND PROSPECTS
The benefits of human recreational activities in the water, including swimming and diving, are well known. Swimming can have beneficial effects on human mental health while strengthening the speed, endurance, strength and flexibility of the body’s organs and muscles. Besides, the benefits of diving include improving blood circulation, helping to release stress, increasing strength and flexibility of muscles and improving human concentration capacity. However, to enjoy the water environment, it is necessary to recognize the limitations of diving or swimming. Swimming and diving may cause many problems for humans. Head-out water immersion or submersion at various depths while diving in water may cause serious cardiorespiratory, endocrine and renal reactions. When swimming, the swimmers are in a horizontal position, in which case the gravitational effects on the circulation system and respiratory physiology change. Under these conditions, breathing is limited to the mechanics of the swimming stroke and the water environment. Under these circumstances, thermoregulatory demands are not balanced with metabolic demands in a water environment with its thermodynamic properties. Blood translocation into the thorax and elevation of plasma volume results in increased cardiac stroke volume and output and affects pulmonary blood flow and gas chambers. Immersion causes an increase in ventilation. Increased blood volume in the lungs leads to capillaries obstruction, which displaces gas volume and may rise the risk of pulmonary edema. When diving in water, especially cold water, the body temperature may drop. In addition, the hydrostatic pressure underwater increases. Under these conditions, compressed gas must be inhaled by a diver, which may lead to oxygen toxicity at high partial pressures, nitrogen narcosis, high pressure nervous syndrome, and problems within the tissue during decompression, bubble formation in the tissues, and carbon dioxide accumulation due to excessive respiration and increased dead space. The evidence suggests that despite the benefits of swimming and diving, activity in aquatic environments is a challenging situation for some organs of the body, especially the respiration physiology comprising respiratory muscles. Some authors believe that swimming with controlled frequency breathing can improve the anaerobic power. This type of breathing prevents swimmers to produce metabolic acidosis but instead the respiratory alkalosis is produced. Some others suggest that the extra respiratory muscle endurance training can improve the parameters of ventilation function, chest expansion, respiratory muscle strength and endurance, as well as swimming performances. According to those researchers studied on diving, calculation of the breath-hold time and diving depth may prevent physiological accidents for divers. Moreover, appropriate insulation is the only protection for the diver against hypothermia. In addition, some researchers recommended that as soon as the body temperature drops below the thermo-neutral temperature, the diver must stop diving and resume it after the body organs have warmed up. An author suggests that by defining inherent limits of oxygen tolerance in diver, appropriate guidelines for safe and efficient applications of hyperoxia in diving operation can be provided. Furthermore, appropriate physiologic function and respiratory system adaptation are important to minimize the dangers associated with diving. The authors’ opinion is that the respiratory muscle fatigue is a physiological action that occurs in many water sports that reduces the capacity of the respiratory muscles to produce energy. This fatigue returns to its original state with rest. Respiratory muscle fatigue can activate the sensory and metabolic reflexes that may affect the performance of the swimmers and divers. The good news is that the respiratory muscles respond to exercise just like any other muscle. If these muscles are properly trained, they can adapt and increase their strength, power and endurance. Similar to the fundamental trainings that exist to strengthen the muscles of the body organs, the respiratory muscles need proper stimulation to make physiological changes in their function and structure. Inspiratory muscle training improves the function of the respiratory muscles through specific resistance exercises and increases the strength, power and endurance of the diaphragm performance and accessory inspiratory muscles and expiratory muscles. Reducing metabolic compounds due to respiratory muscle fatigue can strengthen the respiratory muscles, which ultimately improves the performance of swimmers and divers. The production of metabolic compounds can restrict blood flow to the body organs by stimulating the sympathetic nervous system and vasoconstriction. This causes flow of blood to the respiratory muscles. Blood flow to skeletal muscle is controlled by different effector mechanisms. Neural control is different from humoral, metabolic, endothelial cell and smooth muscle cell control mechanisms. Therefore, strengthening the respiratory system by performing special exercises limits the production of metabolic compounds and reduces the problems raised, which in turn improves the performance of swimmers and divers.
REFERENCES
- Lomax M, McConnell AK (2003) Inspiratory muscle fatigue in swimmers after a single 200m swim. Journal of Sports Sciences 2: 659-664.
- Thomaidis SP, Toubekis AG, Mpousmoukilia SS, Douda HT, Antoniou PD, et al. (2006) Alterations in maximal inspiratory mouth pressure during a 400-m maximum effort front-crawl swimming trial. Journal of Sports Medicine and Physical Fitness 49: 1635-1642.
- Brown S, Kilding AE (2011) Exercise-induced inspiratory muscle fatigue during swimming: the effect of race distance. J Strength Cond Res 25(5): 1204-1209.
- Lomax M, Iggleden C, Tourell A, Castle S, Honey J (2012) Inspiratory muscle fatigue after race-paced swimming is not restricted to the front crawl stroke. Journal of Strength and Conditioning Research 26: 2729- 2733.
- Lomax M, Thomaidis SP, Iggleden C, Toubekis AG, Tiligadas G (2013) The impact of swimming speed on respiratory muscle fatigue during front crawl swimming: a role for critical velocity?. International Journal of Swimming Kinetics 2(1): 3-12.
- Rupp S, Berninger K, Hopf T (1995) Shoulder problems in high level swimmers-impingement, anterior instability, muscular imbalance? International Journal of Sports Medicine 16: 557-562.
- Sein ML, Walton J, Linklater J, Appleyard R, Kirkbride B, et al. (2010) Shoulder pain in Elite swimmers: primarily due to swim-volumeinduced supraspinatus tendinopathy. British Journal of Sports Medicine 44: 105-113.
- Grote K, Lincoln TL, Gamble JG (2004) Hip adductor injury in competitive swimmers. American Journal of Sports Medicine 32: 104-108.
- Stulberg SD, Schulman K, Stuart S, Culp P (1980) Breaststroker’s knee: pathology, etiology and treatment. American Journal of Sports Medicine 8 (3): 164-171.
- Kaneoka K, Shimizu K, Hangai M, Okuwaki T, Mamizuka N, et al. (2007) Lumbar intervertebral disk degeneration in elitecompetitive swimmers: a case control study. American Journal of Sports Medicine 35(8): 1341- 1345.
- Gaunt T, Maffulli N (2012) Soothing suffering swimmers: a systematic review of the epidemiology, diagnosis, treatment and rehabilitation of musculoskeletal injuries in competitive swimmers. British Medical Bulletin 103: 45-88.
- Holmer I (1992) Swimming physiology. The Annals of physiological anthropology 11(3): 269-276.
- Lindholm P, Lundgren CEG (2009) The physiology and pathophysiology of human breath-hold diving. Journal of Applied Physiology 106: 284- 292.
- Epstein M (1976) Cardiovascular and renal effects of head-out water immersion in man. Circulation Research 39(5): 619-628.
- Epstein M (1978) Renal effects of head-out water immersion in man: Implications for an understanding of volume homeostasis. Physiol Rev 58(3): 529-581.
- Chalmers DJ, Morrison L (2003) Epidemiology of non-submersion injuries in aquatic sporting and recreational activities. Sports Medicine 33 (10): 745-770.
- Datta A, Tipton M (2006) Respiratory responses to cold water immersion: neural pathways, interactions, and clinical consequences awake and asleep. J Appl Physiol 100: 2057-2064.
- Tetzlaff K, Thorsen E (2005) Breathing at depth: physiologic and clinical aspects of diving while breathing compressed gas. Clin Chest Med 26: 355-380.
- Bosco G, Rizzato A, Moon RE, Camporesi EM (2018) Environmental physiology and diving medicine. Front Psychol 9: 1-10.
- Viana E, Bentley DJ, Logan-Sprenger HM (2019) A physiological overview of the demands, characteristics, and adaptations of highly trained artistic swimmers: a literature review. Sports Medicine 5: 16.
- Vinetti G, Lopomo NF, Taboni A, Fagoni N, Ferretti G (2020) The current use of wearable sensors to enhance safety and performance in breathhold diving: A systematic review. Diving Hyperb Med 50(1): 54-65.
- Patrician A, Dujić Ž, Spajić B, Drviš I, Ainslie PN (2021) Breath-hold diving - The physiology of diving deep and returning. Frontiers in physiology 12: 639377.
- Rochat I, Côté A, Boulet LP (2022) Determinants of lung function changes in athletic swimmers: A review. Acta Paediatrica 111: 259-264.
- NOAA Diving Manual. 2017. 6th Edn. Best Publishing Company.
- Tu J, Inthavong K, Ahmadi G (2013) Computational fluid and particle dynamics in the human respiratory system. First Edition. Springer, Netherlands.
- Cordain L, Stager J (1988) Pulmonary structure and function in swimming. Sport Med 6: 271-278.
- Wylegala JA, Pendergast DR, Gosselin LE, Warkander DE, Lundgren CEG (2007) Respiratory muscle training improves swimming endurance in divers. European Journal of Applied Physiology 99: 393-404.
- Ferreira MI, Barbosa TM, Costa MJ, Neiva HP, Vilaca J (2016) Effects of swim training on energetic and performance in women masters’ swimmers. Journal of Human Sport & Exercise 11(1): 99-106.
- Lin YC (1988) Applied physiology of diving. Sports Medicine 5: 41-56.
- Pendergast DR, Moon RE, Krasney JJ, Held HE, Zamparo P (2015) Human physiology in an aquatic environment. Comprehensive Physiology 5: 1705-1750.
- Clarys JP (1979) Human morphology and hydrodynamics. In: Terauds J, Bedingfield W (Eds.). Swimming III. University Park Press, Baltimore, Canada, pp. 3-41.
- Clarys JP (1985) Hydrodynamics and electromyography: ergonomics aspects in aquatics. Applied Ergonomics 16: 11-24.
- Toussaint HM, Hollander P, Berg van der C, Vorontsov A (2000) Mechanics and energetics of swimming. In: Garret WE, Kirkendall DT (Eds.). Medical encyclopedia “exercise and sport science”. Lippincott, Williams & Wilkins, Philadelphia, pp. 639-660.
- Seifter JL, Chang HY (2016) Disorders of acid-base balance: new perspectives. Kidney Diseases 2: 170-186.
- Kamel KS, Halperin ML (2017) Chapter 8- Respiratory acid–base disturbances. In Kamel KS, Halperin ML (Eds.). Fluid, Electrolyte and Acid-Base Physiology: A problem-based approach. Fifth Edition. Elsevier, pp. 199-211.
- Vepraskas S, Toth H, Weisgerber M (2018) Chapter 46- Acid-base and electrolyte disturbances. In: Kliegman RM, Lye PS, Bordini B, Toth H, Basel D (Eds.). Nelson Pediatric Symptom-Based Diagnosis. Elsevier, Pp. 831-850.
- Hamm LL, DuBose TD (2020) Chapter 16- Disorders of acid-base balance. In: Alan SL Yu, MB B Chir (Eds.). Brenner and Rector’s The Kidney, 11th edn. Elsevier, pp. 496-536.
- Lemaitre F, Coquart JB, Chavallard F, Castres I, Mucci P, et al. (2013) Effect of additional respiratory muscle endurance training in young well-trained swimmers. Journal of Sports Science and Medicine 12: 630- 638.
- Mijacika T, Dujic Z (2016) Sports-related lung injury during breath-hold diving. European Respiratory Review 25: 506-512.
- Rawlins JSP, Tauber JF (1971) Thermal balance at depth. In: Lambertsen CJ (Ed.) Underwater Physiology. Academic Press, pp 435-442.
- Castellini MA, Kooyman GL, Ponganis PJ (1992) Metabolic rates of freely diving Weddell seals: correlations with oxygen stores, swim velocity and diving duration. Journal of Experimental Biology 165(1): 181-194.
- Knight DR, Horvath SM (1985) Urinary responses to cold temperature during water immersion. American Journal of Physiology-Regulatory, Integrative and Comparative Physiology 248(5): R560-R566.
- Greenleaf JE, Shiraki K, Sagawa S, Miki K, Wada F, et al. (1999) Is the Gauer-Henry reflex important for immersion diuresis in men? Aviation, Space, and Environmental Medicine 70: 1201-1205.
- Choukroun ML, Varene P (1990) Adjustments in oxygen transport during head-out immersion in water at different temperatures. J Appl Physiol 68(4): 1475-1480.
- Clark JM (1988) Pulmonary limits of oxygen tolerance in man. Experimental Lung Research 14: 897-910.
- Schagatay E, Kampen M van, Emanuelsson S, Holm B (2000) Effects of physical and apnea training on apneic time and the diving response in humans. European Journal of Applied Physiology 82: 161-169.
- Andersson JPA, Liner MH, Runow E, Schagatay EKA (2002) Diving response and arterial oxygen saturation during apnea and exercise in breath-hold divers. J Appl Physiol 93: 882-886.
- Lin YC, Lally DA, Moore TO, Hong SK (1974) Physiological and conventional breath-hold breaking points. Journal of Applied Physiology 37(3): 291-296.
- Massery M, Hagins M, Stafford R, Moerchen V, Hodges PW (2013) Effect of airway control by glottal structures on postural stability. Journal of Applied Physiology 115(4): 48-490.
- Du Toit MA, Gray RM (2018) Paraglossal straight blade intubation in syndromic children. Southern African Journal of Anaesthesia and Analgesia 24(5): 118-121.
Article Type
Review Article
Publication history
Received Date: April 14, 2022
Published: May 31, 2022
Address for correspondence
Shaghayegh Doulati Ardejani, Third Faculty of Medicine, Charles University, Czech Republic
Copyright
©2022 Open Access Journal of Biomedical Science, All rights reserved. No part of this content may be reproduced or transmitted in any form or by any means as per the standard guidelines of fair use. Open Access Journal of Biomedical Science is licensed under a Creative Commons Attribution 4.0 International License
How to cite this article
Shaghayegh Doulati A, Saleem N. Respiratory Physiology in Swimming and Diving: A Literature Review. 2022- 4(3) OAJBS.ID.000454.