Morbidity Associated with Infectious Diseases in Children Under 5 Years in Selected Public and Private Sector Hospitals of Peshawar
ABSTRACT
Introduction: Infectious diseases are disorders caused by organisms- such as bacteria, viruses, fungi or parasites. Many
organisms live in and on our bodies. They’re normally harmless or even helpful, but under certain conditions, some organisms may
cause disease. The infectious diseases may be bacterial, viral, fungal, parasitic. Infectious diseases can be caused by bacteria.
Objectives:
1. To identify morbidity rate due to infectious diseases in children under 5 years.
2.To collect data from the previous record of morbidity rate due to infectious diseases in public and public sector hospitals in
Peshawar.
3.To compare the rate of morbidity between private and public sector hospitals in Peshawar.
4.To determine the most prevalent disease in children below five years in Peshawar.
Materials and Methods: The study was carried out in the months of October to March at two private hospitals (RMI and
NWGH) and two public sector hospitals (KTH and HMC) of Peshawar Pakistan. We randomly selected 100 children from these
hospitals who were suffering from infectious diseases.
Results: This cross-sectional study showed that the disease with the highest number of cases was pneumonia (36%), which is
followed by RDS (21%) and diarrhea (17%). Relation of an education status of parents with vaccination and prevalence of disease
was also of significance as 58 % fathers were literate, with 42% illiterates whereas 56% mothers were literate and 44% of them
were illiterate.
Conclusion: The finding of this study shows that ratio of infectious diseases was high in children of illiterate people and rate of
infectious diseases was low in vaccinated children.
KEYWORDS
Infectious diseases; Pneumonia; Children; Diarrhea; Private sector; Vaccine
INTRODUCTION
Bacterial, viral and fungal invasion causes diseases termed as infectious diseases. Some of them reside in our bodies and are mainly harmless however may get harmful whenever the situation is favorable. The infectious diseases may be bacterial, viral, fungal and parasitic. Infectious diseases can be caused by Bacteria. These organisms manifest as upper respiratory tract infections, urinary tract infections and gastrointestinal infections. Parasites may be transmitted to humans from animal feces. Leading causes of morbidity and mortality vary from developing to developed countries with infectious diseases being the leading cause in former and accidents being the leading cause in later. Pakistan is eighth among the countries, who bear 95% of the burden of infectious diseases where less than five, less than one year and less than one month mortality is 97, 78 and 57 per 1,000 live births. The main cause of death therefore in 70% children is infectious diseases. Nearly two million children less than five years of age die of pneumonia. Similar number dies of diarrhea every year. Pneumonia and diarrhea collectively are responsible for 22% of all childhood mortality in Pakistan, mortality because of measles is 20,000 deaths in children annually. Measles vaccine coverage is lowest among all EPI vaccines (60% nationwide, with Sindh province having the lowest coverage i.e. 20%). Other than these Tuberculosis and Tetanus are also among the leading causes of death with numbers rising remarkably.
The objectives of our research were to identify the morbidity rate due to infectious diseases, to collect data about morbidity rate, to compare morbidity rate between public and private sector hospitals in Peshawar and to determine the most prevalent infectious diseases in children less than 5 years. Pakistan is among the six countries which bear 95% burden of malarial disease with children being the prime victim [1]. The research article was published in global journal of research and review which is Diarrhea among Children Under Five Years in Ghana in 2017, the result of this research showed that Diarrhea was least found in children between 0-6 months (5.6%) because they were usually exclusively breastfed, in the Ghanaian communities, so less exposed to contaminated food. Diarrhea occurs in both males and females but more common in males the prevalence of diarrhea in males was 13.1% and 10.2% in females [Constitutional factors: Biological factor such as food antigens found in cow’s milk, soya, egg, proteins and nuts were likely to cause allergic response in children which may cause diarrhea [2].
The research article (Concurrent Pneumonia in Children Under 5 Years of Age Presenting to a Diarrheal Hospital in Dhaka, Bangladesh) was conducted in Dhaka, Bangladesh which shows that respiratory and gastrointestinal infections were the top killers of children worldwide, their aim was to determine the risk factors for concurrent presentation of diarrhea and pneumonia (DP). It was found out that those with DP had a higher mortality rate 4% versus 0.05%, odds ratio [OR] = 86, 95% confidence interval [CI] = 26-286) and a longer hospital stay (mean 84 versus 26 hours, difference 58 hours, 95% CI = 52-64 hours) than those with diarrhea (D) only [3]. Another study at Thailand stated that among the 49% with chest radiographs, 76% had findings of pneumonia. The hospitalized ALRI incidence rate was 5772 per 100,000 childyears and was higher in boys versus girl and in children 6-23 months of age versus other age groups. Most common viruses responsible for ALRI were respiratory syncytial virus (19.5%), rhinoviruses (18.7%), bocavirus (12.8%) and influenza viruses (8%). Bloodstream infections, most commonly Streptococcus pneumonia and typhoid, Salmonella, accounted for 1.8% of cases [4]. Another study at Tunisia which shows that a total of 10,797 RTD patients were enrolled from 49,880 pediatric hospitalizations (21.7%). A male predominance was noted (60%). The median age was 8 months. Acute bronchitis (AB) accounted for 53.8%, followed by asthma (15%), pneumonia (14%) and acute upper respiratory infection (AURI; 7.2%). The hospital had 34/10 000 inhabitants/ year incidence rate of RTD. Projected trends analysis up to 2024 showed a significant rise in AB and in asthma, while AURI would significantly decrease [5].
A research article showed that in developing countries infectious disease are still the leading cause of morbidity and mortality in children. This is contrary to the developed countries where injuries are the leading cause of death and disabilities [6]. Similar systematic review on the incubation period and period of infectiousness showed that on average, 5 days of exclusion is considered for measles, mumps, rubella, varicella and pertussis. For other diseases, such as most cases of meningococcal disease, hepatitis A and influenza exclusion is considered if severe symptoms persist [7].
The research about global Illness and Deaths Caused by Rotavirus Disease in Children is done in 2003 an estimated 125 million infants 0–11 months of age and 450 million children 1–4 years of age reside in developing countries. A systemic review of 27 studies of 20 countries from 1990 to 2000 projected those children less than 11 month of age had 3.8 diarrheal episodes per child per year and children 1 to 4 years of age had 2.1 diarrheal episodes per child per year. Multiplying these age-specific incidence data with the population of children in each age group yielded an overall estimate of approximately 1.4 billion diarrhea episodes per year in children <5 years of age. Of these, 475 million episodes are estimated to occur in <11-month-old infants and 945 million episodes in children 1–4 years of age [8].
Keeping in view the importance of infectious diseases, this descriptive study is conducted to compare the morbidity rate due to infectious diseases among children under 5 years in the selected hospitals of Peshawar. So that specific diseases could be highlighted which have high rate of morbidity and by comparison between two sectors of hospitals services could be implemented according to sector which has less rate. The aim of the study is to find out morbidity rate due to infectious diseases occurring in KPK in children under 5 years and how they could be treated and prevented.
MATERIALS AND METHODS
The study was carried out in the months of October to March at two private hospitals (RMI and NWGH) and two public sector hospitals (KTH and HMC) of Peshawar Pakistan. We randomly selected 100 children from these hospitals who were suffering from infectious diseases. These children were under 5 years old and were suffering from pneumonia, diarrhea, respiratory tract infections, malaria, RDS and other common infectious diseases. Participants were divided into different groups on the basis of type of infectious disease and age group of the patients. Parents of these children participated in our research and cooperated with us as a lot of children suffers from infectious diseases in this region and people really want to get rid of this. This data was collected by using the interview-based questioners and parents of patients were interviewed by members of this research project and data was analyzed by using the IBM SPSS Statistics Data Editor Version 10.
The study design was comparative observational study. Our study includes children under 5 years both male and female, suffering from infectious diseases in selected private and public sector hospitals and all those children suffering from infectious diseases with any other physical or psychological illness, the incorrect or incomplete questionnaires, noncooperative and none consenting guardians will be excluded.
RESULTS
This Table 1 shows that majority (32%) patients belonged to NWGH, while only 18% belonged to RMI. Regarding the age of the patients 64% patients were under the age of 1 day to 11 months, while only 4 % patients belonged to the age group 4 to 5 years. Regarding the gender 60 % of the patients were males and 40% were females. 58% of fathers and 56% of mothers of the patients were educated. 80% of patients belonged to urban areas and 20 % belonged to rural.
This Table 2 shows that disease with the highest number of cases (36%) is pneumonia, which is followed by RDS (21%) and diarrhea (17%). The diseases with least number of cases were Dysentery, Viral meningitis and PCM (protein calorie malnutrition) that is 1% each.
This Table 3 shows that most of the patients (68%) were vaccinated till date, while 26% were not vaccinated at all. The remaining 6% were incompletely vaccinated till date.
This Table 4 shows that the significance between age and vaccination was 0.028. This shows that the relation is very significant.
Table 5,6 shows the significance between education of father and mother vaccination came out to be 0.702, which is not significant.
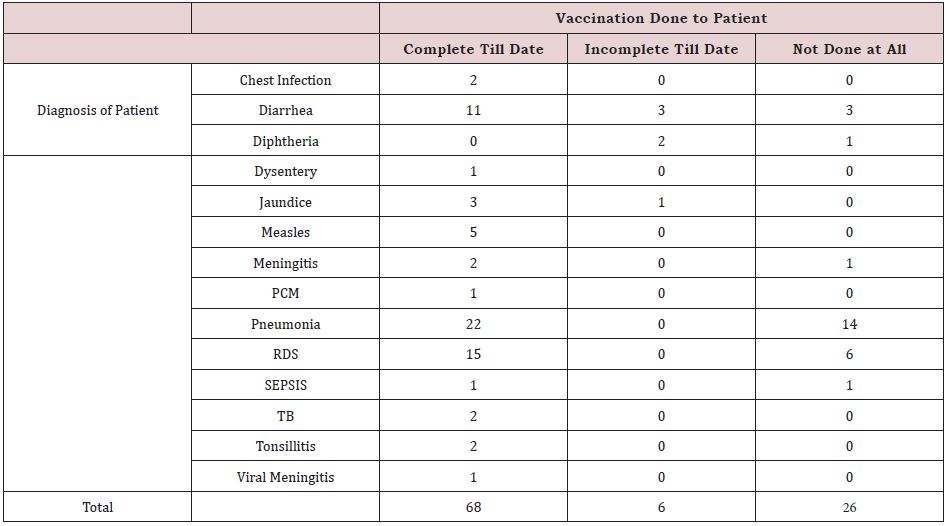
This Table 7 shows the significance between diagnosis and vaccination came out to be 0.025. This shows that the value is very significant (Figure 1).
DISCUSSION
According to our result, the disease with the highest number of cases was pneumonia (36%), which is followed by RDS (21%) and diarrhea (17%). The diseases with least number of cases were Dysentery, Viral meningitis and PCM (protein calorie malnutrition) that is 1% each. Vaccination is completed in cases of pneumonia and RDS, while in cases of diarrhea vaccination was incomplete. Relation of education status of parents with vaccination and prevalence of disease was also of significance as 58 % fathers were literate, with 42% illiterates whereas 56% mothers were literate and 44% of them were illiterate .In accordance to our study, a study conducted at Bangladesh, Dhaka showed that respiratory and gastrointestinal infection were the major contributors as out of total 14,628 diarrheal patient surveyed, there were 607 (4%) patient who satisfied criteria for pneumonia likewise we also found that diarrhea and pneumonia were associated with children under 5, male gender, severe acute malnutrition and less maternal education.(3)Literacy have role in diseases prevention, while in our findings the literacy rate is considerably less. In accordance to our study, a study conducted at urban slum of Gulbarga city showed that 109 children giving an incident of 27.25%, among these URT was found 19.25% and LRT 8%. ARI was observed among 38.04% of infants, 37.84% of 2-3-year-old children, 36.87% of boys, 40.43% of children born to illiterate fathers. (9) A similar study was done where 51.8% died of preterm birth complication and pneumonia (14.9%). In contrary to our study, a study conducted at Nigeria showed that out of 3830 children more than 70% were under 5 years of age. The common indications for admission were malaria (30.3%), diarrheal diseases (20.4%), respiratory tract infections (RTIs) (19.0%) and sepsis (4.4%). (10) Another study contrary to ours conducted at Tunisia where a total of 10797 patients were enrolled from pediatric hospitalization, the highest number of cases (53.8%) acute bronchitis, followed by asthma 15%, pneumonia 14% and upper respiratory infection 17%. This significant increase in pneumonia in our result is probably due to environmental changes, incomplete vaccination and illiteracy. The aim of the following study was to limit the morbidity of children under 5 years admitted at pediatric ward of selected private and public sector hospitals as to provide an insight of a broader picture and to tackle them on a regional basis.
LIMITATIONS
It was not possible to stay at the hospital all the time so, we considered the data of patients only present at pediatric wards and did not include the patients present in gynae and other wards for our convenience. Secondly, our sample size was small so we could not cover all the patients that suffered from infectious diseases.
CONCLUSION
The finding of this study shows that ratio of infectious diseases was high in children of illiterate people and rate of infectious diseases was low in vaccinated children.
RECOMMENDATIONS
We considered our research based on generalized cases of infectious diseases. So, our recommendation to new researchers would be to conduct research based on endemic infectious diseases of their area. This will prove valuable for the accuracy of their result.
REFERENCES
- Aisha M (2009) Infectious diseases in children-still leads. J Pak Med Assoc 59(7): 425-426.
- Ameyaw R, Ameyaw E, Acheampong AO, Appiagyei P (2017) Diarrhea among children under five year in Ghana. Glob J Res Rev 4(2).
- Leung DT, Das SK, Malek MA, Qadri F, Faruque AS, et al. (2015) Concurrent Pneumonia in Children Under 5 Years of Age Presenting to a Diarrheal Hospital in Dhaka, Bangladesh. Am J Trop Med Hyg 93(4): 831- 835.
- Hasan R, Rhodes J, Thamthitiwat S, Olsen SJ, Prapasiri P, et al. (2014) Incidence and etiology of acute lower respiratory tract infections in hospitalized children younger than 5 years in rural Thailand. Pediatr Infect Dis J 33(2): e45-e52.
- Ben AH, Yaïch S, Ben JM, Jedidi J, Ben HM, et al. (2017) Pediatric respiratory tract diseases: Chronological trends and perspectives. Pediatr Int 60(1): 76-82.
- Traebert J, Nickel DA, Traebert E, Escalante JJ, Schneider (2016) The burden of infectious diseases in the Brazilian Southern state of Santa Catarina. J Infect Public Health 9(2): 181-191.
- Ida C, Chantal Q, Pierluigi L, Jan CS (2018) Management and control of communicable diseases in schools and other childcare settings: systematic review on the incubation period and period of infectiousness. BMC Infect Dis 18(1): 199.
- Umesh DP, Erik GH, Joseph SB, Mark AM, Roger GI (2003) Global illness and deaths caused by rotavirus disease in children. Emerg Infect Dis 9(5): 565-572.
- Ramani VK, Pattankar J, Puttahonnappa SK (2016) Acute Respiratory Infections among Under-Five Age Group Children at Urban Slums of Gulbarga City: A Longitudinal Study. J Clin Diagn Res 10(5): LC08-LC13.
- Ezeonwu BU, Chima OU, Oguonu T, Ikefuna AN, Nwafor I (2014) Morbidity and mortality pattern of childhood illnesses seen at the children emergency unit of federal medical center, Asaba, Nigeria. Ann Med Health Sci Res 4(Suppl 3): S239-S244.
Article Type
Research Article
Publication history
Received Date: September 09, 2022
Published: September 26, 2022
Address for correspondence
Nouman Antony, Rehman Medical institute Peshawar, Pakistan
Copyright
©2022 Open Access Journal of Biomedical Science, All rights reserved. No part of this content may be reproduced or transmitted in any form or by any means as per the standard guidelines of fair use. Open Access Journal of Biomedical Science is licensed under a Creative Commons Attribution 4.0 International License
How to cite this article
Moula G, Nouman A, Jibran U, Muhammad ZAC, Mamoon UR, Muhammad AYK, Muhammad S, Salman A. Morbidity Associated with Infectious Diseases in Children Under 5 Years in Selected Public and Private Sector Hospitals of Peshawar. 2022- 4(5) OAJBS.ID.000489.
Table 1: Demographic data.
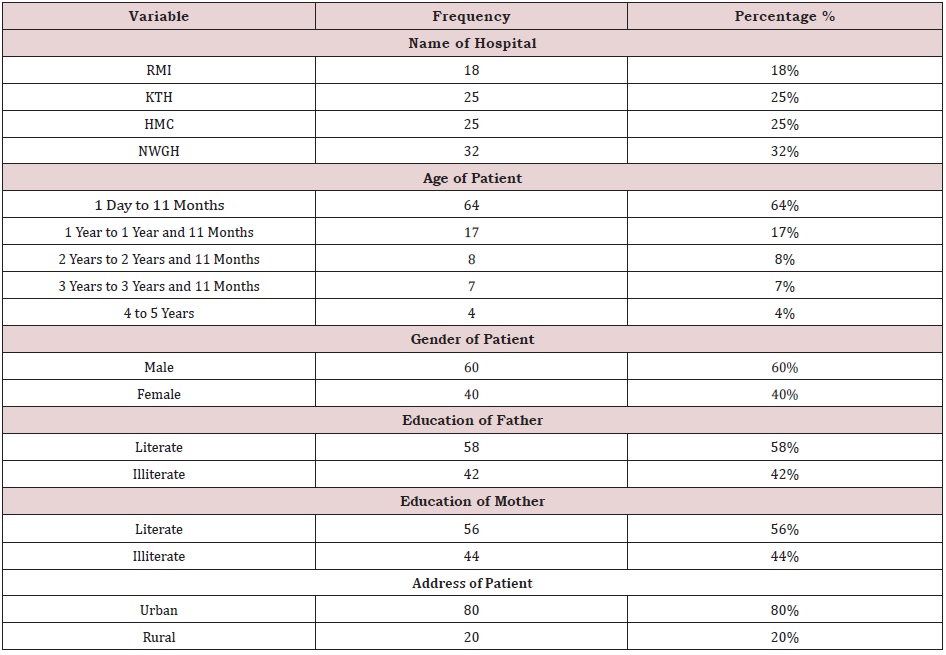
Table 2: Frequencies of diagnosis.
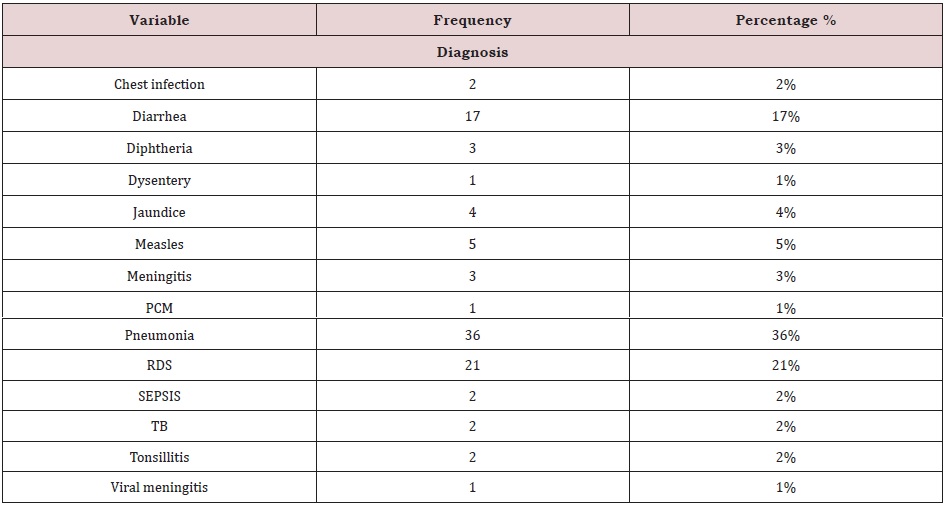
Table 3: Vaccine profile.

Table 4: Age to vaccination cross tabulation.
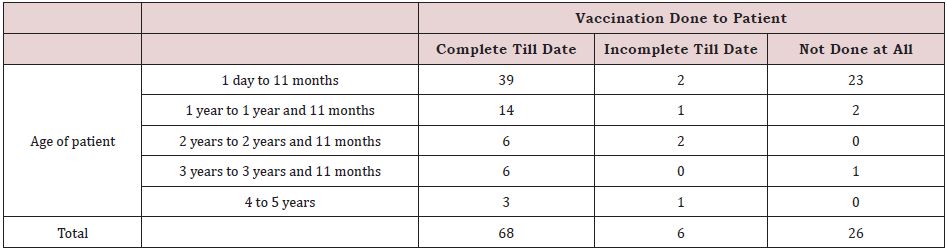
Table 5: Education of father to vaccination cross tabulation.

Table 6: Education of mother to vaccination cross tabulation.

Table 7: Diagnosis of patients to vaccination cross tabulation.