Factors Affecting Stroke Knowledge and Awareness in Emergency Patients in Izmir City
ABSTRACT
Objectives: Knowing stroke risk factors and recognizing stroke warning signs are critical for reaching both to preventive and emergency stroke treatments. In this study, we aimed to evaluate the stroke knowledge and perceptions of the people who live in Izmir province and to determine the factors affecting their awareness.
Methods: This is a multicentre population-based survey. The number of participants was determined by simple random sampling method. Volunteers who had applied to the emergency services and gave consent for participation were enrolled into the study, consecutively. The questionnaire was filled out by face-to-face interviews at the hospital by professional interviewers.
Results: Most of the participants were female and lived in the urban areas. 39% had stroke story in their family. 32.8% had at
least one risk factor. The most frequently observed risk factor among the participants was smoking (42.7%). One-third of participants
did not know which organ’s dysfunction caused stroke. 84% of participants reported that the level of their knowledge about stroke
was insufficient. One-fifth of participants believed that stroke was a consequence of evil spirits. Paralysis or weakness of one side
of the body (93.8%) was determined as most known stroke warning sign. Primary sources of information were family and friends.
Conclusion: We showed that there is insufficiency in knowledge and awareness about stroke risk factors and recognition of
warning signs. Community based education programs using mass media will be effective in meeting the need for knowledge and in
reaching larger communities.
KEYWORDS
Awareness; Emergency department; Knowledge; Perception; Population-Based survey; Stroke
INTRODUCTION
Stroke is an important public health problem that can cause death or disability [1-3]. According to 2017 Turkey Statistical Institute report, death caused by circulatory system diseases is in the first place. 22.9% of deaths were caused by cerebrovascular diseases [4]. Prevention involves distinct determination and control of risk factors. Good recognition of findings and early arrival to health center may decrease mortality and morbidity [5,6]. Knowing stroke risk factors and recognizing warning signs are associated with knowledge and perception level of the population [2-6]. This awareness level affects both the success of primary preventive therapies and access to emergency interventions [2,3,7- 9]. Population based studies in USA, Australia, Canada, Brazil, India, Iran, Jordan, Uganda and Nigeria showed lack of population knowledge on stroke risk factors and warning signs. Literature survey showed only one study done by Evcil et al. [2] on-population knowledge and perception of stroke, in Turkey [2].
OBJECTIVE
Emergency departments (ED) are the primary healthcare areas most frequently encountering stroke patients. We aimed to evaluate the stroke knowledge and perception of emergency patients and factors affecting their awareness, attitude, and behaviour in presence of stroke suspicion.
MATERIALS AND METHODS
Study Design
This is a community-based, multicentre survey study. Local ethical committee approval was obtained (Local Ethics Committee Meeting No: 5, Approval Date and Ordinance No: 13.07.2017/31).
Study Population
Adult patients who applied to the ED and with an Emergency Severity Index [14] triage rating 5 were included in the study consecutively. Surveys were conducted between 09.00-11.00 AM and 20.00-22.00 PM. Patients unwilling to participate and those with communication difficulty (such as active complaints, mental illness, hearing and/or speech impairment, language difference, or inability to speak) were excluded.
Sample Size
Number of participants was determined by using “simple random sampling” method. Total population of İzmir province was accepted as 3.506.366, and the sample size was determined to be 400 people, at least. Homogenous data collection was achieved by dividing İzmir provenance into two regions as North and South. Hospitals where the survey would be implemented determined by the consideration of populations, mean age and number of ED admissions in these districts. The number of participants to be included in the study from any related hospital was determined with the annual total number of ED patient admissions of that hospital.
Survey
The questionnaire was structured after reviewing relevant literature studies [2,3,5,7,9,12]. In the preliminary study, final version of the questionnaire was formed by interviewing 42 people who were not included in the study. The study was divided into 4 main sections.
Demographic characteristics: Age, gender, habitat, education status, medical history, and habits (risk factors of patients) were questioned.
Factors Affecting Stroke Awareness
a) Stroke perceptions and experiences were evaluated by asking two answer optioned closed-ended questions like yes/no or sufficient/insufficient. Knowing what stroke is, stroke history of themselves or relatives, stroke knowledge level, and reasons that caused stroke were questioned. Cause of stroke perception and beliefs were grouped under titles of supernatural causes (bad spirits, evil eye, and demons), brain hemorrhage, vascular occlusion, heart disease, diabetes, hypertension, rhythm disorder, poor hygiene, and poor nutrition
.b) Participants’ knowledge about stroke: Knowing stroke risk factors, warning signs and basic clinical features were evaluated by asking diversified questions.
The sources of information about stroke were evaluated by open-ended question.
Reaction attitudes and behaviors in suspicion of stroke were evaluated by asking multiple response open-ended questions.
Choosing Reference Standards
Hypertension, stress, heart disease, genetic predisposition, high cholesterol, smoking, diabetes mellitus, alcohol dependence, obesity, malnutrition, cancer, and poor hygiene were considered as risk factors in our study. Ten different symptoms were selected from the definitive focal, non-specific focal and global stroke symptoms [1]. These were facial asymmetry, weakness in one half of the body, speech disorders (aphasia, dysphasia), visual disturbances (double vision, vision loss, and fixed gaze), headache, change in consciousness, and lethargy. In our study, the most correct and effective behavior in case of stroke suspicion was accepted as the activation of 112 Emergency Medical System (EMS). Also, ‘’the organ being affected causes stroke?’’.
STATISTICAL ANALYSIS
Suitability of the data with normal distribution was evaluated with the Shapiro-Wilk Normality test. Descriptive statistics were summarized by mean ± standard deviation or median (min-max), frequency and percentage, in accordance with the distribution. Chisquare test was used to compare categorical variables in groups, and Mann Whitney U test was used for continuous variables. IBM SPSS for Windows Ver. 20, (Statistical Package for Social Sciences, IBM Inc., Illinois-USA®) program was used for all statistical analysis and p value of <0.05 was considered significant.
RESULTS
Volunteers of 485 agreed to participate of which 53.6% were female, 60.8% were living in urban area, and 30% were living alone. The mean age was 41.46 ± 14.25 years, and 30% were university graduates. A significant decrease was observed in education level as the age increased (p<0.001). Participants of 67% had different risk factors (one in 32.8% and more than one in 34.2%). Males had more risk factors. The first three most common risk factors were smoking (42.7%), hypertension (19.2%), and diabetes (13.6%), respectively.
RESULTS
Stroke Perception and Experience
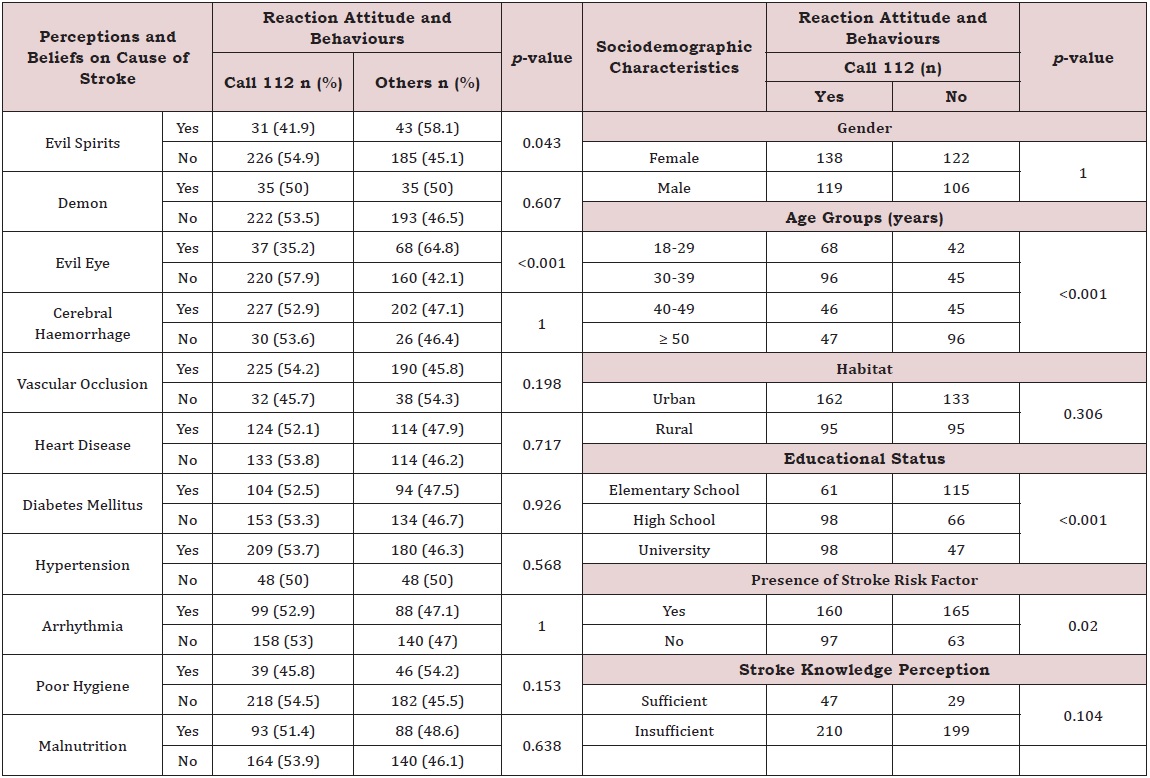
Only 5 (1%) of the volunteers had a stroke. 298 people (39%) had a stroke story in their family or relatives, often described their knowledge of stroke as sufficient (p=0.26). Most participants (93%) stated that they knew what stroke was whereas 84% described their knowledge as insufficient. Participants who described their stroke knowledge level as sufficient were mostly university graduates (40.8%). The organ dysfunction that caused stroke was answered wrong by 32.4%, and the 18-29 age group were significantly unsuccessful (p=0.04). At least one stroke risk factor was in 85% of participants. No relation was found between having stroke risk factor and stroke knowledge and perception (p=0.589). Most frequent answer to stroke cause was brain hemorrhage (88.5%). Also, 21.6% believed in evil eye, 14.4% in bad spirits, and 15.3% in demons as the cause of stroke. Males mostly stated hypertension (76.4%), and females reported brain hemorrhage (89.2%) as the cause of stroke. Belief in supernatural causes was significantly more frequent among the participants aged 50 and over with literation and primary school education who lived in rural areas (p=0.001; p=0.001; and p=0.001, respectively). Belief of bad spirit caused stroke in participants with risk factors was twice as much of others (p=0.011). Participants who described their stroke knowledge as sufficient more frequently defined vascular occlusion as a cause of stroke (p=0.012); (Table 1)..
Stroke Knowledge
The participants of 13.6% reported that they knew stroke risk factors (sufficient: 8.4%; insufficient: 5.2%). The most commonly known risk factors by participants were hypertension (83.3%), stress (76.1%) and heart disease (55.1%). The least known risk factors were poor hygiene (16.5%), cancer (17.5%) and poor nutrition (34.4%). Smoking was not defined as a risk factor by 53.6%. The most commonly known stroke warning sign was weakness in one half of the body (93.8%) whereas the least known was headache (28.5%). Among the warning signs of stroke, speech disorders were known with 93.2%, asymmetry on face 91.1%, numbness 62.9%, change in consciousness 61% and visual impairments 44.3%. Participants aged 50 and over knew the symptoms of visual impairment and change in consciousness more frequently (p<0.001, p<0.001, respectively), whereas literate and elementary school graduates knew the visual warning signs more frequently (p=0.004). Participants who defined their stroke knowledge as sufficient, knew the signs; visual impairment (p=0.023), headache (p=0.001), change in consciousness (p=0.007) and numbness (p=0.009) significantly more (Table 2).
Female knew that stroke was preventable (p=0.044), and participants aged 50 and over knew of its sequelae feature (p=0.035) more frequently. Literate and primary school graduates knew more about the sequelae feature (p=0.003) whereas university graduates knew the early recognizable features more often (p<0.001). The rate of knowing recurrence feature among literate and primary school graduates was significantly low (p=0.004). However, participants who defined their stroke knowledge as sufficient knew more on difficulty/inability to perform basic daily activities after stroke, only (p=0.003); (Table 3).
Stroke Information Sources
Family and friends were the most common sources of information on stroke (56.5%). The rate of information acquisition from television (TV) was 48.9%, doctors 33.4%, internet 27.2% and newspapers 13%. It was determined that TV (p=0.002) and, family and friends (p=0.023) were used more frequently as a source of information in the 50 and over age group, whereas internet was more frequent in the 30-39 age group (p<0.001). Participants living both in urban (85.6%) and rural (56.3%) areas stated that the sources of information were often family and friends. It was determined that the participants living in the rural areas benefited more from TV (p=0.015) and newspapers (p=0.031) and those living in the urban areas more from doctors, significantly (p=0.038).
It was found that the literate and primary school graduate participants acquired information more from families and friends (p=0.035) and the university graduates more from newspapers, internet, and doctors (newspapers: 20.7%, p=0.001; internet: 55.9%, p<0.001 and doctors: 49%, p<0.001, respectively). Participants defining knowledge as sufficient were acquiring information from doctors, mostly (p=0.003), and those as insufficient from TV (p=0.046). No significant relation was found between having a stroke risk factor and sources of information (p=0.589); (Table 4).
Reaction Attitude and Behaviours in Suspicion of Stroke
Only 53% of participants replied “I would call 112” in suspicion of stroke. Participants aged 50 and over, stated to call 112 significantly less (p<0,001) whereas the ratio was higher in 30-39 age group. The ratio of university graduates to call 112 was significantly higher than other education level groups (p<0.001). Participants who did not have a risk factor had a significantly higher attitude to call 112 than those with one or more risk factors (p0.001)./0.001).=0.020); (Table 5). Participants who thought stroke was due to bad spirits and evil eye, showed a lower attitude to call 112 (p<0.001); Table 5.
DISCUSSION
Factors Affecting Stroke Awareness
Stroke perception and experiences: In their study, Madae’en et al. [13]; Haghighi et al. [6] reported the rates of participants who had a stroke as 1.5% and 4.2%, respectively. In our study, stroke rate was 1% and rate of participants with a stroke story in family or relatives was much lower (39% vs 63.8%, 93% respectively). Contrary to Falavigna’s et al. [11] report, a significant relationship between the presence of a stroke history in the family and the stroke knowledge levels of the participants was found, similar to the study of Yoon et al. [15].
In our study, the rate of knowing which organ being affected caused stroke was close to that of Evcil’s et al. [2] study (68.6% vs 64.5%). Compared to international literature, our rate was lower than the rates reported by Madae’en et al. [13]; Yoon et al. [15]; Falavigna et al. [11] and higher than those reported by Akinyemi et al. [5]; Pandian et al. [12] (68.6% vs 75%, 73.4%, 70.5%, 28.7%, 45% respectively). Nakibuuka [7] reported that knowing the correct answer for the organ affected by stroke, was related to well knowing the warning signs of stroke. Falavigna et al. [11]; Pancioli et al. [16] reported that both low socio-economic level and low education status are independent factors related with the wrong answer. However, Madae’en et al. [13], reported that knowing neither which organ being affected, nor the symptoms of stroke had a relationship with gender and education status.
Age was determined as an important factor to know which organ being affected causes stroke. It is thought that the lack of information of the young age group is due to disinterest. Furthermore, significant relationship observed between the high education level and the knowledge of stroke being sufficient. 93% of participants who stated knowing what stroke is and answered brain hemorrhage as a cause, at a high rate, was considered incompatible with their knowledge of stroke definition as insufficient and less knowing which organ being affected causes stroke. This contrast may be due to the diversified open-ended questions and closedended questions in which participants could choose more than one answer. Therefore, some questions about stroke awareness may be overestimated. Jones et al. [17] reported, review of 39 studies investigating stroke knowledge and awareness, differences in questioning techniques may affect answers. In addition, open-ended questions were not as precise in determining stroke symptoms and risk factors as close-ended questions.
In African origin studies, it has been stated that stroke-like symptoms thought to be caused by natural or environmental factors, as well as of supernatural causes such as demons and sorcery [7-18]. Evaluation of similar supernatural causes in publications from countries with high index of development was not found.
Akinyemi et al. [5] reported that most frequent answer to stroke occurrence was due to vascular occlusion, 65%, similar to the population-based study reported from Ireland, 60% [19]. Akinyemi consisted of answers from healthcare professionals and reported that being a health worker and having a higher education level was more effective in knowing the causes of stroke [5].
Basic knowledge about stroke
Yoon et al. [20] reported that 76% of the participants could list at least one risk factor for stroke, Akinyemi et al. [5] 68.1% Evcil et al. [2] 63.6%. In our study, 13.6% replied ‘‘yes’’ to knowing the risk factors. Although, an exceedingly small group stated knowing the risk factors, it was observed that risk factors were known at high rates when evaluated one by one. This way of asking questions was similar with the assisted, closed-ended questioning technique that Jones et al. [17] recommended. It was foreseen that this method would facilitate determination of which risk factors are less known and how to develop training programs with respect to missing information.
Hypertension has been reported as the most commonly known risk factor, ranging from 56% to 93.6% in many studies [5-7,11]. The most known risk factor in our study was also hypertension. Nakibuuka et al. [7] attributed it to the frequent occurrence of the disease in the community. In contrast, Yoon et al. [3] reported that the most known risk factor in his studies was smoking, in Evcil et al. [2] stress, and in Madae’en’ et al. [13] advanced age and story of stroke. Participants who stated not knowing stroke risk factors were mostly felt having insufficient information. However, it was also found that those who felt having sufficient information also did not know the risk factors enough. For example, smoking was not identified by 53.6% of the participants in our study. This finding was interpreted as if the participants neglected or were unaware of the risk factors they had.
Nakibuuka et al. [7] reported that knowing stroke warning signs and risk factors is related to having a high education level and having diabetes whereas Haghighi et al. [8] reported that the stroke knowledge of the participants was not related to the level of education and race. Falavigna et al. [11], on the other hand, defined that being younger than 50 years old and having low socioeconomic level was associated with insufficient knowledge of stroke risk factors and as a risk.
The frequency of knowing at least one stroke warning sign has been reported at different rates, such as, 85.5%, 57%, and 50% [3,16,20]. The rate of knowing more than one stroke warning sign was reported at rates ranging from 8% to 28% (16.20). In the studies of Parahoo et al. [19]; Akinyemi et al. [5]; Pandian et al. [12]; Evcil et al. [2] weakness in one half of the body is reported to be the most commonly known stroke warning sign (91%, 61.9%, 60.2%, and 37.1% respectively). On the contrary, Madae’en et al. [13]; Yoon et al. [3] reported that speech disorders are the first (62% and 60.1%, respectively) and weakness in one half of the body is the second mostly known warning signs (52.6% and 42%, respectively). In our study, the first two stroke warning signs to be known most frequently were weakness in one half of the body and speech disorders, respectively. However, the rate of knowing these two signs was higher than all the aforementioned studies. This may be a result due to the technique of asking questions which was reported in the study of Jones et al. [17].
Akinyemi et al. [5]; Yoon et al. [3] reported that knowing the warning signs of stroke was related to higher education level. Yoon et al. [3] also reported that other sociodemographic characteristics and having a risk factor is not related to knowing the warning signs of stroke. Similarly, no relationship between the level of stroke knowledge, perception and having a risk factor was found in our study. However, it was observed that being over 50 years with a low education level has negative correlation with knowing the stroke warning signs, whereas defining level of knowledge as sufficient and having high education level has a positive correlation. This result was explained with the fact that participants who felt their level of stroke perception was sufficient, was mostly composed of highly educated ones reaching multiple sources of information.
In the literature, very few studies were conducted on the basic clinical features of stroke. Yoon et al. [3] reported that participants of young age and highly educated groups knew the basic features of stroke more than those aged 40 and over. Evcil et al. [2]; Yoon et al. [3] reported, once more, that the most frequent known properties of stroke were recurrence and being preventable.
In our study, Females knowing stroke being a preventable disease in higher rate was related to the high number of female participants. Furthermore, participants aged 50 and over, and those with low education level knew more about the sequelae feature was interpreted as increased possibility to encounter it throughout their long lifetimes. Again, the fact that participants, high education level and defined knowledge as sufficient, knew more on early recognition, recurrence and difficulty/inability to do basic daily activities after stroke was linked to their preference in reliable information sources. The fact that both the participants with advanced age and low education level, and all who defined knowledge as sufficient and have high education level, knew the basic clinical features of stroke was interpreted with relation of question asking technique.
Information Sources About Stroke
It has been reported that information about stroke can be successfully increased using media sources [21]. It was also reported that participants who were informed by doctors on their risk factors knew more on their stroke probability [3]. In our study, it was found that the highly educated group acquired more information from doctors than other participants and that these participants defined their stroke knowledge as sufficient, more frequently.
Reaction Attitude and Behaviors in Suspicion of Stroke
In their studies, Madae’en et al. [13]; Akinyemi et al. [5]; Nakibuuka et al. [7] reported the rate of attitude to activate 112 EMS in suspicion of stroke as 85%, 90%, 80% respectively. In our study, this rate was 53% and as the level of education increased, the attitude to activate EMS increased significantly, whereas it decreased with increasing age.
Alberts et al. [22] reported that patients with cerebral infarction provided a significant improvement in their admission time after a community education program that used a multimedia approach. In the first 24 hours, the rates of direct or via referral transportation to a hospital increased from 37% to 86% after the program. Similarly, Stern et al. [21] reported that they achieved a 10.9% increase in stroke awareness and knowledge between the pre and the post-education group.
It has been reported that community reactions should be planned appropriately, and a comprehensive multi-approach strategy is needed to protect people from first stroke attacks and provide hospital admissions right after the symptoms appear [3]. In the same study, it was emphasized to find methods of education and motivation to reduce risk factors and to educate patients about risk factors from primary care.
LIMITATIONS
The distribution of the education level of the participants may be not reflecting that of province of Izmir. Some questions on factors affecting stroke awareness may be mostly guessed due to differences in the technique of asking questions. Despite similar practices in many studies, the understanding of the questions asked, and the answers received may have been limited in older and less educated people. The results of this study cannot be generalized for the entire population of Turkey or another population.
CONCLUSION
Our study showed that there is great necessity in increasing knowledge and awareness about knowing the risk factors of stroke, recognizing warning symptoms and what to do if a stroke is suspected. The main causes of poor stroke knowledge can be summarized as being too young or old, low educational level, and not using accurate information resources, enough. TV and newspapers can be generalized to be the best tools for public education. The public should be regularly informed via educational and cautionary public spots and program broadcasts about the risk factors and warning signs of stroke, and what to do when stroke is suspected. In fact, education should be spread throughout school age and primary health care.
ACKNOWLEDGEMENT
We would like to thank Okan Sayan for his help in language editing.
INFORMED CONSENT
Informed consent was observed verbally for the present study before conducting the survey.
ETHICAL APPROVAL
Ethical approval to report this retrospective study was obtained from University of Health Sciences, Tepecik Educational and Research Hospital, Local Institutional Ethical Committee (Approval date and no; 13.07.2017/31).
ETHICAL CLEARANCE CERTIFICATE/HUMAN RIGHTS
Our work does not infringe on any rights of others, including privacy rights, and intellectual property rights. There is no human rights violation in our manuscript.
AVAILABILITY OF DATA AND MATERIALS
The datasets analysed during the current study are available from corresponding author.
AUTHOR CONTRIBUTIONS
The authors: Dr. M.S. and U.T. conceived the study, designed the trial. Dr. N.Y.O., Y.E. and U.T. supervised the conduct of the trial and supervised the data collection. Dr. O.G., Y.E., N.Y.O., N.K. managed the patients’ data, including quality control. PhD. A.S. provided statistical advice on study design and analysed the data; Dr Sever chaired the data oversight committee. Dr. M.S. and U.T. were drafted the manuscript, and all authors contributed substantially to its revision. Dr. MS. is revising it critically for important intellectual content and final approval of the version to be submitted. Dr M.S. takes responsibility for the paper as a whole. All authors have read and approved the final version of the submitted manuscript.
REFERENCES
- World Health Organization (2006) WHO steps-stroke manual: The WHO Stepwise approach to stroke surveillance.
- Evcil ED, Memis S, Ergin F, Beser E (2007) A population-based study on awareness of stroke in Turkey. European Journal of Neurology 14(5): 517-522.
- Sug Yoon S, Heller RF, Levi C, Wiggers J (2001) Knowledge and perception about stroke among an Australian urban population. BMC Public Health 1:14.
- (2017) Turkish Statistical Institute. Statistics of cause of death. Turkish Statistical Institute Newsletter.
- Akinyemi RO, Ogah OS, Ogundipe RF, Oyesola OA, Oyadoke AA, et al. (2009) Knowledge and perception of stroke amongst hospital workers in an African community. European Journal of Neurology 16(9): 998-1003.
- Borhani Haghighi A, Karimi AA, Amiri A, Ghaffarpasand F (2010) Knowledge and attitude towards stroke risk factors, warning symptoms and treatment in an Iranian population. Med Princ Pract 19: 468-472.
- Nakibuuka J, Sajatovic M, Katabira E, Ddumba E, Byakika-Tusiime J, et al. (2014) Knowledge and perception of stroke: a population-based survey in Uganda. ISRN Stroke.
- Greenlund KJ, Neff LJ, Zheng ZJ, Keenan NL, Giles WH, et al. (2003) Low public recognition of major stroke symptoms. American Journal of Preventive Medicine 25: 315-319.
- Kaddumukasa M, Kayimal J, Kaddumukasa MN, Ddumba E, Mugenyi L, et al. (2015) Knowledge, attitudes and perceptions of stroke: a crosssectional survey in rural and urban Uganda. BMC Res Notes 8: 819.
- Ramsden VR, Shuaib A, Reeder BA, Khan K, Liu L (1994) Risk factor awareness: a randomized telephone survey of public knowledge. Can J Public Health 85(suppl2): 57-60.
- Falavigna A, Teles AR, Vedana VM, Kleber FD, Mosena G, et al. (2009) Awareness of stroke risk factors and warning signs in Southern Brazil. Arq Neuropsiquiatr 67(4): 1076-1081.
- Pandian JD, Jaison A, Deepak SS, Kalra G, Shamsher S, et al. (2005) Public awareness of warning symptoms, risk factors and treatment of stroke in Northwest India. Stroke 36: 644-648.
- Madae’en SS, Bulatova NR, Al-Qhewii TA, Sakran LH, El-Zayyat HH, et al. (2013) Stroke awareness in the general population: a study from Jordan. Trop J Pharm Res 12(6): 1071-1076.
- Gilboy N, Tanabe T, Travers D, Rosenau AM (2011) Emergency Severity Index (ESI): A triage tool for emergency department care, Version (4th edn). Implementation Handbook 2012. AHRQ publication, USA.
- Yoon SS, Byles J (2002) Perceptions of stroke in the public and patients with stroke: a qualitative study. BMJ 324: 1065-1068.
- Pancioli AM, Broderick J, Kothari R, Brott T, Tuchfarber A, et al. (1998) Public perception of stroke warning signs and knowledge of potential risk factors. JAMA 279(16): 1288-1292.
- Jones SP, Jenkinson AJ, Leathley MJ, Watkins CL (2009) Stroke knowledge and awareness: an integrative review of the evidence. Age Ageing 39(1): 11-22.
- Bham Z, Ross E (2005) Traditional and western medicine: cultural beliefs and practices of South African Indian Muslims with regard to stroke. Ethn Dis 15(4): 548-554.
- Parahoo K, Thompson K, Cooper M, Stringer M, Ennis E, et al. (2003) Stroke: awareness of the signs, symptoms and risk factors: a populationbased survey. Cerebrovasc Dis16: 134-140.
- Sug Yoon S, Heller RF, Levi C, Wiggers J, Fitzgerald PE (2001) Knowledge of stroke risk factors, warning symptoms and treatment among an Australian urban population. Stroke 32(8): 1926-1930.
- Stern EB, Berman M, Thomas JJ, Klassen AC (1999) Community education for stroke awareness: an efficacy study. Stroke 30(4): 720-723.
- Alberts MJ, Perry A, Dawson DV, Bertels C (1992) Effects of public and professional education on reducing the delay in presentation and referral of stroke patients. Stroke 23(3): 352-356.
Article Type
Research Article
Publication history
Received Date: October 29, 2022
Published: November 21, 2022
Address for correspondence
Mustafa Sever, Associate Professor of Emergency Medicine, University of Health Sciences, Tepecik Educational and Research Hospital, Department of Emergency Medicine, Turkey
Copyright
©2022 Open Access Journal of Biomedical Science, All rights reserved. No part of this content may be reproduced or transmitted in any form or by any means as per the standard guidelines of fair use. Open Access Journal of Biomedical Science is licensed under a Creative Commons Attribution 4.0 International License
How to cite this article
Ufuk T, Mustafa S, Necmiye YO, Yesim E, Olcay G, Asli S, Nezih K. Factors Affecting Stroke Knowledge and Awareness in Emergency Patients in Izmir City. 2022- 4(6) OAJBS. ID.000518. DOI: 10.38125/OAJBS.000518
Table 1: Relationships between sociodemographic characteristics and stroke perceptions and beliefs.
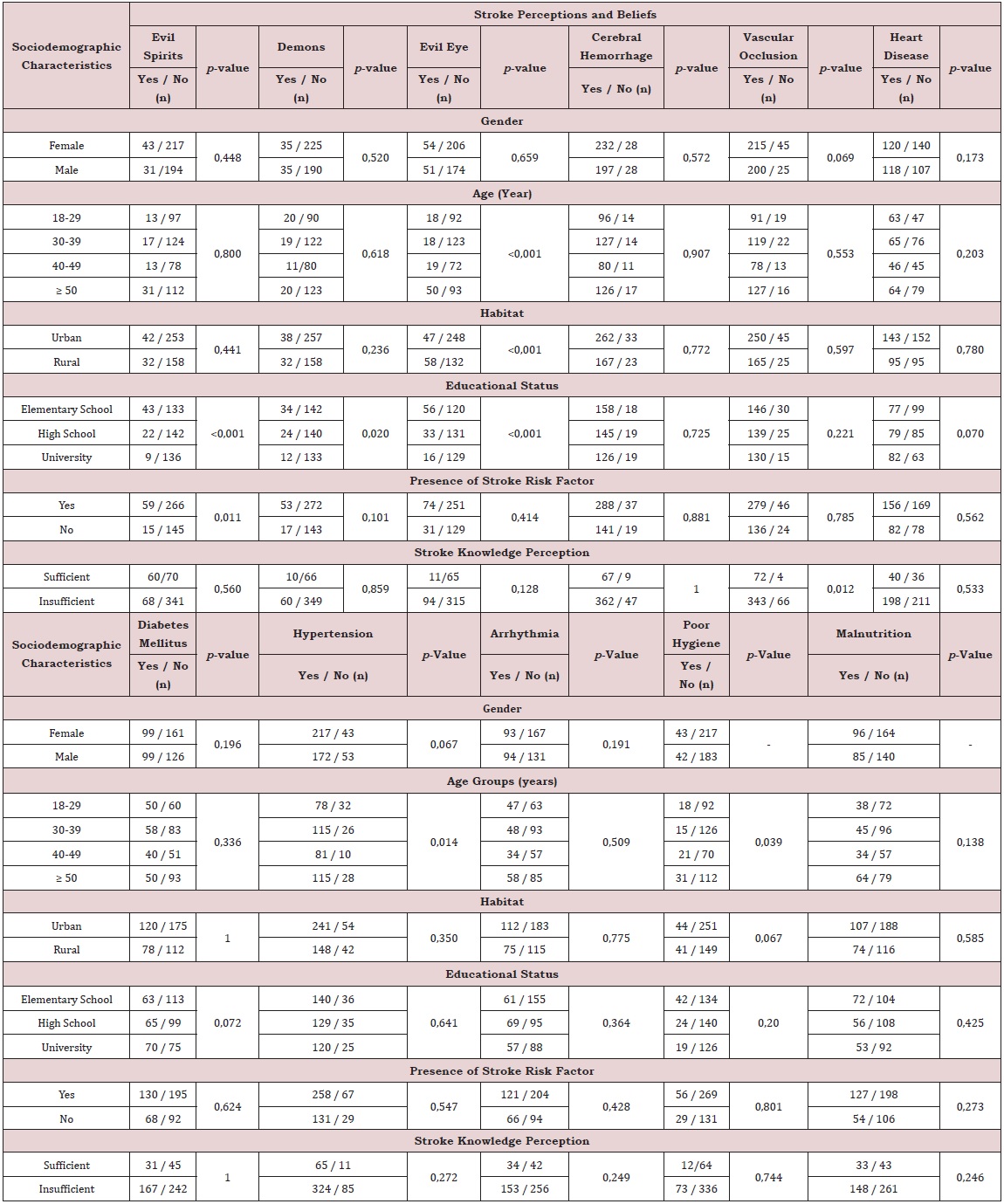
Table 2: Relationships between sociodemographic characteristics and knowledge of stroke warning signs.
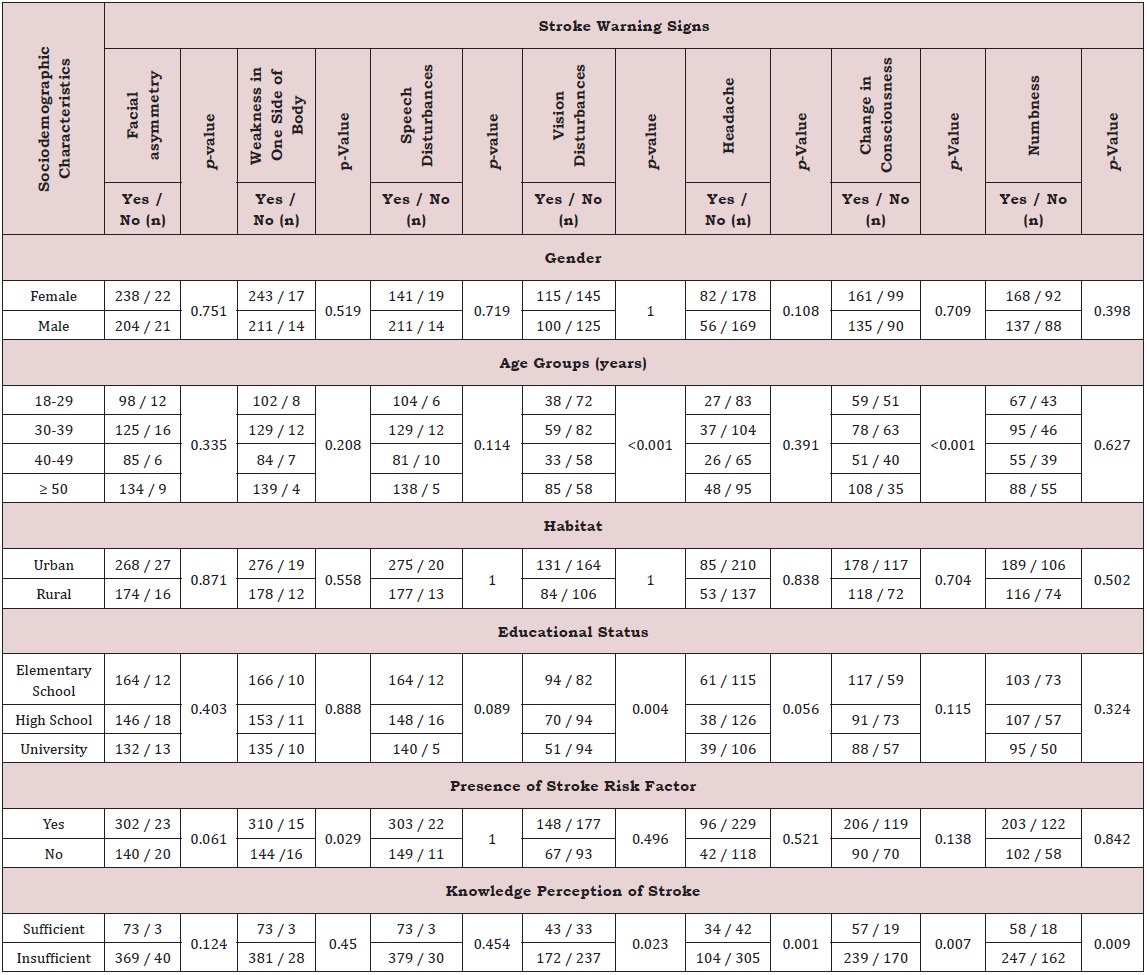
Table 3: Relationships between sociodemographic characteristics and knowledge of basic clinical features of stroke.
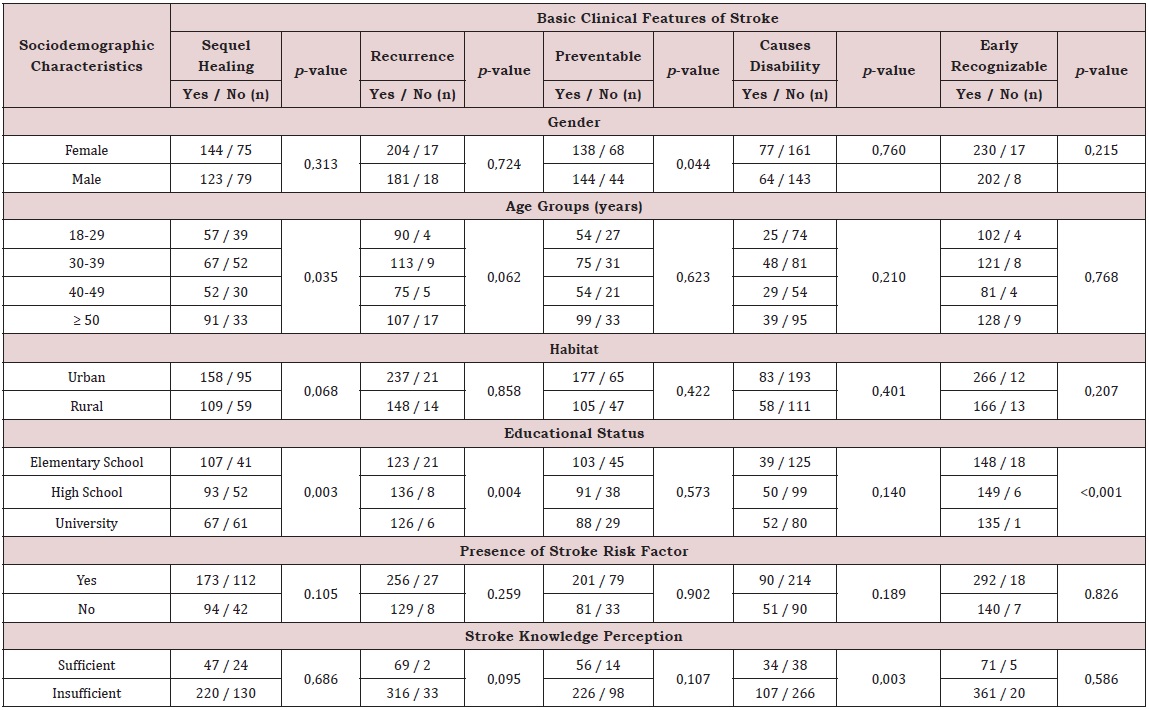
Table 4: Relationships between sociodemographic characteristics and sources of information. [8].
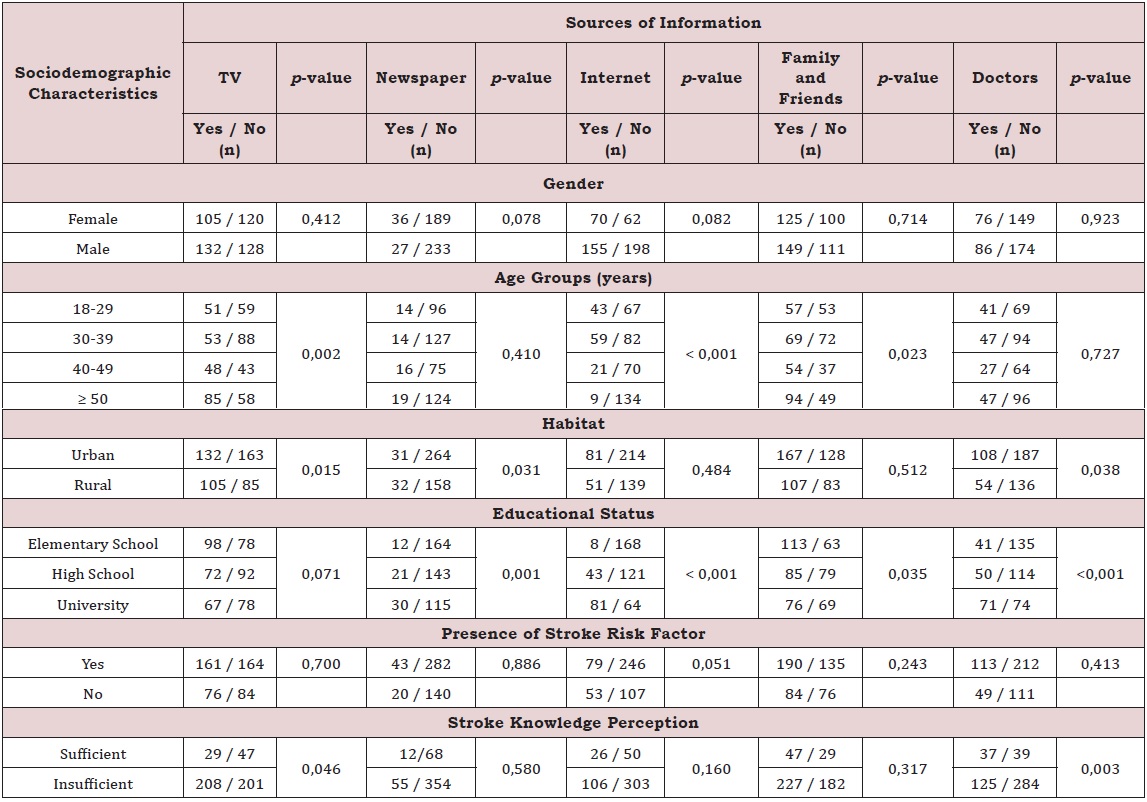
Table 5: Relation attitude and behaviours according to stroke perceptions and beliefs and sociodemographic characteristics in stroke suspicion. [8].