Anxiety and Depression Scores in Patients with Coronary Heart Disease and Hypertension
ABSTRACT
Background: Higher incidence of hypertension has been repeatedly documented in patients with depression, and hypertension
is a well-known risk factor of coronary heart disease (CHD). Interestingly, depression is considered to be independently associated
with a significantly increased risk of CHD. Considering the intriguing and risk-multiplying relationships among depression,
hypertension and CHD, we assessed the anxiety and depression scores in CHD patients with or without hypertension.
Materials and Methods: 388 CHD patients (163 cases comorbid with hypertension, 225 cases not) from department of
cardiology in Jining first people’s hospital were included. Depression scores were assessed with the Patient Health Questionnaire-9
(PHQ-9), and anxiety scores via Generalized Anxiety Disorder 7-item scale (GAD-7).
Results: No statistically significant differences were noticed between CHD patients with and without hypertension in terms
of clinical characteristics such as age, gender, BMI, smoking and drinking status. In CHD patients with hypertension, GAD-7 scores
were significantly higher than patients with only CHD (P<0.001). Additionally, there also was a significant difference of GAD-7 scores
between these two groups for both males (P<0.01) and females (P<0.05). Similarly, PHQ-9 scores were significantly higher in CHD
patients with hypertension than patients with only CHD (P<0.001) and the differences were significant in both genders.
Conclusion: Our study demonstrated that GAD-7 and PHQ-9 scores were elevated in CHD patients comorbid with hypertension,
indicating that hypertension is a major risk of depression and anxiety, which may also worsen the CHD condition.
KEYWORDS
Coronary disease; Hypertension; Depressive disorder; Patient health questionnaire
ABBREVIATIONS
CHD: Coronary Heart Disease; PHQ-9: Patient Health Questionnaire-9; GAD-7: Generalized Anxiety Disorder 7-Item Scale
INTRODUCTION
Coronary heart disease (CHD) is one of the leading causes of global burden of disease, being an issue in which both public and private health systems spend large amounts of money every year. The adverse cardiovascular outcomes and heavy health care costs portend high prevalence of psychological factors, such as depression and anxiety. Conversely, meta-analysis also suggests that depression is independently associated with a significantly increased risk of CHD [1].
Interestingly, there is a growing body of evidence describing increased prevalence of hypertension in depressed patients [2,3]. In turn, prospective studies have also suggested that high scores of depressive symptoms doubled the risk for hypertension [4] and increased prevalence of depression has been described in hypertensive patients as well [5]. Additionally, hypertension is a well-known risk factor of coronary heart disease (CHD) [6].
Considering CHD, hypertension and depression being ranked as the leading causes of worldwide burden of disease, clarifying the relationship among them will have a relevant big impact on both clinical environment and public health. Therefore, to better understand the common causal pathways and help us delineate more appropriate treatments, we evaluated the mental scores in CHD patients with or without hypertension.
MATERIALS AND METHODS
Subjects
Between October 2015 and January 2017, 388 CHD patients were recruited at the outpatient clinic of cardiology in Jining first people’s hospital of Shandong Province based on the Diagnostic criteria described in previous research [7]. In brief, CHD was defined as the presence of coronary artery stenosis greater than 50% for at least one of the three major coronary arteries or major branches. All participants included in our study had no history of significant concomitant diseases, including severe hepatic and renal diseases, bleeding disorders, previous thoracic irradiation therapy, and malignant diseases. Among them, 225 patients were diagnosed with CHD only and 163 patients were diagnosed with CHD comorbid with hypertension. The protocol was approved by the Ethics Committee of Jining First People’s Hospital, and written informed consents or finger prints were obtained from all participants prior to the research.
Evaluation of GAD-7 and PHQ-9
Generalized Anxiety Disorder 7-item scale (GAD-7) is a selfreport scale whose scores can reach values from 0-21, with a cut off values higher than 4 [8]. Likewise, Patient Health Questionnaire-9 (PHQ-9) is a 9-item questionnaire with possible values from 0 to 27 and a cut-off of 4 [9]. The GAD-7 [10] and PHQ-9 [11] questionnaires have an excellent validity and reliability for the diagnosis of anxiety and depression, respectively, which were widely used to evaluate the psychological and physical symptoms of anxiety and depression in adults. To minimize the environmental factors, the questionnaires including GAD-7 and PHQ-9 were self-completed by the participants in a separate room unless they asked for help to write or read.
Statistical Analysis
Continuous variables were compared by using independent sample t test, and categorical data analysis was carried with a Chi-square test. The level of P<0.05 was prespecified for all tests of significance, which were two-tailed. All statistical analysis was performed in SPSS version 19.0.
RESULTS
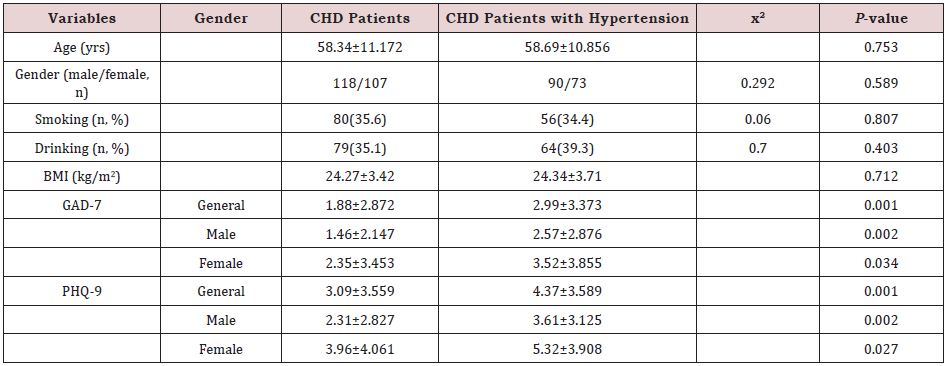
The clinical characteristics (age of onset, gender, smoking and drinking) and mental scores of patients were listed in (Table 1). Patients with only CHD did not differ from CHD patients comorbid with hypertension with regard to all tested demographic variables, such as age of onset, gender, smoking and drinking status. In CHD patients with hypertension, GAD-7 scores were significantly higher than patients with only CHD (P<0.001). Moreover, there also was a significant difference of GAD-7 scores between these two groups for both males (P<0.01) and females (P<0.05). Likewise, PHQ-9 scores were significantly higher in CHD patients with hypertension than patients with only CHD (P<0.001) and the differences were significant in both genders.
To further assess the relationship among mental disorder, hypertension and CHD, all patients in this study were identified as having anxiety or depression if their total GAD-7 or PHQ-9 score was ≥ 5, respectively. Statistical data compared by Chi-square test indicated that the prevalence of anxiety increased from 12.4% (28/225) in CHD patients to 20.2% (33/163) in CHD patients comorbid with hypertension (x2=4.341, P=0.037, OR: 1.786; 95% CI: 1.030-3.096). Likewise, the prevalence of depression increased from 27.1% (61/225) in CHD patients to 38.0% (62/163) in CHD patients comorbid with hypertension (x2=5.211, P=0.022, OR: 1.650; 95% CI: 1.072-2.541).
DISCUSSION
Substantial data have indicated that psychiatric conditions and hypertension are closely related [12]. Mental disorders, including depression and anxiety, are risk factors for the development of hypertension, and hypertension can lead to the occurrence of mental disorders in return. Our study suggested that hypertension is associated with the increased risk of anxiety and depression in CHD patients. Consistent with our findings, [5] found a 3-fold higher frequency of major depression in patients treated for hypertension, confirming the increased prevalence of depression in hypertensive patients [5]. Moreover, prospective study in Finland demonstrated that hopelessness was associated with increased incidence of hypertension in 616 initially normotensive men [13], suggesting a critical link between the two conditions. As a well-known leading risk factor for CHD, hypertension makes an important contribution to the mortality of CHD patients, and thus the control of hypertension is particularly critical for CHD patients. Considering the close relationship between depression and hypertension, it is important to take psychic factor into consideration and the intervention of anxiety and depression may be effective for the control of hypertension in CHD patients.
CONCLUSION
In brief, we have investigated the anxiety and depression scores in CHD patients with hypertension, indicating that hypertension is a major risk of depression, which may also worsen the CHD condition. Our study was limited by small sample size and regional biases despite of excluding other environmental factors. Therefore, large-scale studies on physiological mechanism are warranted to be conducted to clarify the relationship among anxiety, depression and hypertension in CHD patients.
ACKNOWLEGEMENT
The study was supported by the Natural Science Foundation of Shandong Province (No. ZR2020QH166; No. ZR2020QH270; No. ZR2020MH375).
CONTRIBUTIONS
Co-authors: Hailiang Zhang and Wenxiu Han have contributed equally to this work.
REFERENCES
- Gan Y, Gong Y, Tong X, Sun H, Cong Y, et al. (2014) Depression and the risk of coronary heart disease: a meta-analysis of prospective cohort studies. BMC Psychiatry 14: 371.
- Adamis D, Ball C (2000) Physical morbidity in elderly psychiatric inpatients: prevalence and possible relations between the major mental disorders and physical illness. Int J Geriatr Psychiatry 15: 248-53.
- Nakagawara M, Witzke W, Matussek N (1987) Hypertension in depression. Psychiatry Res 21: 85-6.
- Jonas BS, Franks P, Ingram DD (1997) Are symptoms of anxiety and depression risk factors for hypertension? Longitudinal evidence from the National Health and Nutrition Examination Survey I Epidemiologic Follow-up Study. Arch Fam Med 6: 43-49.
- Rabkin JG, Charles E, Kass F (1983) Hypertension and DSM-III depression in psychiatric outpatients. Am J Psychiatry 140: 1072-1074.
- Zhang JX, Dong HZ, Chen BW, Cong HL, Xu J (2016) Characteristics of coronary arterial lesions in patients with coronary heart disease and hypertension. Springer Plus 5(1): 1208.
- Liu ZX, Ji HH, Yao MP, Wang L, Wang Y, et al. (2019) Serum Metrnl is associated with the presence and severity of coronary artery disease. J Cell Mol Med 23: 271-280.
- Spitzer RL, Kroenke K, Williams JB, Lowe B (2006) A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med 166: 1092-1097.
- Kroenke K, Spitzer RL, Williams JB (2001) The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med 16(9): 606-613.
- Löwe B, Decker O, Müller S, Brähler E, Schellberg D, et al. (2008) Validation and standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the general population. Med Care 46: 266-274.
- Du N, Yu K, Ye Y, Chen S (2017) Validity study of Patient Health Questionnaire-9 items for Internet screening in depression among Chinese university students. Asia Pac Psychiatry 9.
- Graham N, Smith DJ (2016) Comorbidity of depression and anxiety disorders in patients with hypertension. J Hypertens 34: 397-398.
- Everson SA, Kaplan GA, Goldberg DE, Salonen JT (2000) Hypertension incidence is predicted by high levels of hopelessness in Finnish men. Hypertension 35: 561-567.
Article Type
Research Article
Publication history
Received Date: May 19, 2022
Published: August 10, 2022
Address for correspondence
Fang Yuan and Yujin Guo, Institute of Clinical Pharmacy & Pharmacology, Jining First People’s Hospital, Jining Medical University, China
Copyright
©2022 Open Access Journal of Biomedical Science, All rights reserved. No part of this content may be reproduced or transmitted in any form or by any means as per the standard guidelines of fair use. Open Access Journal of Biomedical Science is licensed under a Creative Commons Attribution 4.0 International License
How to cite this article
Wenxiu Han, Hailiang Zhang, Pei Jiang, Fang Yuan, Yujin Guo. Anxiety and Depression Scores in Patients with Coronary Heart Disease and Hypertension. 2022- 4(4) OAJBS. ID.000478.