A Peer Group Education Intervention to Improve Awareness, Knowledge and Preventive Behavioral Intentions for Pelvic Inflammatory Disease (PID) Among Rural Communities in South-Eastern Nigeria
ABSTRACT
Background: Calls for cost effective interventions towards STIs are never ending. Therefore, studies have suggested peer
education intervention as a cost-effective approach in raising awareness, improving knowledge and encouraging preventive
behaviors against STIs. While women are particularly at risk of contracting STIs, those in the rural communities are at a greater risk
of having them due to their low socio-economic status and high illiteracy level. In this study, we focused on an aspect of STI that have
often been neglected in interventions: Pelvic Inflammatory Disease (PID). Specifically, the study examined the effectiveness of Peer
group education intervention on awareness, knowledge and preventive behavioral intentions towards PID among women in rural
communities.
Methodology: A quasi-experimental research design was conducted on 338 women in both treatment and control communities.
Results: the study found that peer education intervention was effective in raising awareness, improving knowledge and
preventive behavioral intentions towards PID among women in rural communities.
Conclusion: Because PID issues do not draw as much scholarly attention as other STIs in literature, there is a great need to begin
to focus on the disease that is silently affecting a number of women of childbearing everywhere.
KEYWORDS
Pelvic inflammatory disease; Rural women; Young women; Peer education; intervention effect
INTRODUCTION
The purpose of this study was to examine the efficacy of peer group education intervention on Pelvic Inflammatory disease for women of reproductive age in rural communities. The choice of rural communities was based on the fact women in these areas are particularly at a higher risk of contracting sexually transmitted infections as well as experiencing complications that comes with such infections. Two important reasons exist to explain this situation. First, there are a great number of illiterate women with low socioeconomic status in rural communities. Such level of illiteracy according to Ezeah et al. [1] makes it difficult for them to access crucial health information on traditional media such as TV, radio, magazine and newspaper. Secondly, there is a lack of healthcare facilities [1], which could have been a ready source of information with respect to sexual health in rural communities. This becomes worse in environment where there is no peer educator programmed to improve women’s awareness and knowledge about their sexual health. As a result, we are of the opinion that peer educators can address the obvious lack of access to information on STIs and particularly PID issues in rural communities where the use of traditional media could sometimes be costly, hence the need for the study.
Peer group education refers to some type of information transfer, the focus of which is to promote certain kind of behaviors. In this case, there is a peer educator who serves as a source of knowledge and inspiration for the other members of the group. Also, there is a close match between the peer group educator and his/her team members in terms of age, gender, and other considerations. Despite the proliferation of both traditional (TV, radio, Newspaper and Magazine) and new media (Internet and social media), which have given rise to a decrease in face-to-face interaction, this kind of close contact communication is important and unavoidable because it is not possible for people not to communicate physically [1]. It is because of these advantages that many researchers have adopted peer group education intervention in promoting preventive behaviors against STIs and other sexual health challenges. For example, in their evaluation of the effectiveness of peer education in improving knowledge, attitude and preventive behavior regarding HIV among adolescents in Osun state Nigeria, Adeomi et al. [2] found that following peer education intervention, there was an increase in knowledge and positive attitudes towards HIV/AIDs improved significantly. Bulduk [3] investigated the impact of HIV/STIs peer education on knowledge, prevention efficacy and risky sexual behavior among a group of sexually active Turkish students who were not using condom. They found that peer education reduced risky sexual behavior among students. Their result also revealed that significant differences exist according to group by time interaction in the variables of HIV knowledge, self-efficacy for condom use and refusing sexual intercourse. Their studies conclude that peer education is effective in improving knowledge, attitude and preventive behaviors towards STIs [2,4]. Also, in a systematic review designed to evaluate the effectiveness of peer education groups on improving sexual health knowledge and reducing sexual health risks in college campuses, Wong et al. [5] revealed that peer education intervention motivated students to increase condom use and adopt frequent HIV testing behavior. This significant improvement was particularly observed among women, according to the authors. Despite studies showing the efficacy of peer group education on STIs preventive practices, integrated review and meta-analyses have shown mixed outcomes indicating that such intervention might or might not be useful [6,7]. Although there is evidence to suggest that peer education programs are moderately effective in developing countries, their effects on biological outcomes are not statistically significant.
General preventive measures against a disease like PID include practicing safe sex and abstinence. Other educational efforts have also focused on teaching patients to always get tested along with their partners and recommending that women do not douche. The potentials of these measures to address STIs including PID have been highlighted in literature. While some studies on condom use [8] have identified an association between the practice of consistent condom use and prevention of PID among women, other research have found that not having multiple sexual partners and going for regular screening could reduce a woman’s chances of contracting PID [7]. However, evidence shows lack of association between frequent douching and development of PID [8]. Unlike the case of HIV, Gonorrhea, etc., studies examining the impact of peer group education intervention on PID awareness, knowledge and preventive practices are scanty. Available studies on the effectiveness of peer intervention have mostly focused on chlamydia disease [3,8]. Which could lead to PID when left untreated. As a result, we hypothesized that:
a) Peer group education intervention will be effective in creating awareness on PID among rural communities. b) Peer group education intervention will be effective in improving the knowledge level of PID among rural communities. c) Peer group education intervention will be effective in improving preventive behavioral intentions against PID development among rural communities.
METHODS
A quasi-experimental design was used to measure the effect of peer group education intervention on awareness, knowledge and preventive behavioral intentions against PID development. We obtained an ethical clearance from the Health Research Ethics Committee (HREC) which is the institutional review body domicile at the University of Nigeria Teaching Hospital, Ituku-Ozalla, Enugu, Nigeria. A priori power analyses were conducted with the G*power program. This was done to determine whether the sample was adequate. The parameters were set with power (1-β) at 0.90, 0.25 effect size f, and α=.05. The results indicated that a total sample size of 338 participants was needed to detect statistical differences at the .05. A total of 169 control group and 169 intervention group took part in the study. The mean age for the control group was 33.4 years (range: 21-44 years), while the mean age for the intervention group was 32.0 years (range: 19-46 years).
Treatment Procedure
The study was conducted in Edem Ani, Nsukka Local Government Area of Enugu State. The study area is made up of three autonomous communities known as Akpa-Edem (consisting of 13 villages), Ozi-Edem (consisting of 14 villages) and Edem- Ani (consisting of 14 villages). Furthermore, the research team purposively selected two (i.e., Ozi-Edem and Edem-Ani-consisting of 14 villages each) of the three autonomous communities to partake in the study. While Edem-Ani served as the treatment community, Ozi-Edem was chosen as the control community. Also, a team of individuals from the target group was recruited as peer educators. The team was recruited through self-nomination and target audience nomination. The peer educators received briefing from health experts on the basic information (i.e., Who is susceptible, behaviors that make these women susceptible, ways of preventing and receiving treatment for PID) that the group should know about PID. There were 15 members team who spent 14 days interacting with women in the treatment community, informing and imparting the knowledge of PID on them. Another 15-member group of peer educators was recruited to ‘teach’ the control community on general issues of hygiene that do not relate with PID. The researchers instructed peer educators to avoid discussing issues they were taught with women from another community.
Sampling
The researchers adopted a simple random sampling technique in selecting women into both treatment and control groups. This technique was considered appropriate because of its capacity to make generalizations across the population under focus. Participants were represented from each of the 14 villages in each of the communities under study. A self-designed structured questionnaire was used to elicit data from the participants. Peer group educators administered the questionnaires to the participants. The peer educators translated the questions into the native dialect of the people. This enabled the women to answer the questions appropriately. The questionnaire was divided into three major parts: ‘awareness of PID’, ‘knowledge of PID’ and ‘behavioral intentions towards PID prevention. The questionnaire was presented using a four-point Likert scale ranging from: 4= ‘strongly agree’, 3= ‘agree’, 2= ‘disagree’ and 1= ‘strongly disagree’. Examples of items or statements on the questionnaire include, ‘Having pain in the pelvis, lower back or abdomen is a sign that a woman has PID’, ‘I know what a woman can do to prevent PID’, ‘I don’t have unprotected sex because I need to prevent a disease like PID’, ‘I intend to have a single sexual partner and as I believe that it can prevent me from contracting PID’, etc. A reliable Cronbach’s alpha (α) of .71, .89, and .92 were obtained for each of the scales (‘awareness of PID’, ‘knowledge of PID’, and ‘behavioral intentions towards PID prevention’) respectively. It should be noted that the questionnaire was administered before and after the peer education intervention took place.
Measuring Effect
Peer educator intervention effect on awareness of PID, knowledge of PID, and behavioral intentions was measured by comparing the outcome of both the treatment and control communities at baseline and after the two-week exposure to peer education on PID. An improvement in the mean scores of women’s awareness, knowledge and behavioral intentions towards PID prevention after exposure to peer education training on PID compared to scores at the baseline would suggest that the intervention might have worked.
Data Analysis
A Statistical Package for Social Sciences (SPSS) version 23 was used for data analysis. The researchers employed both descriptive and inferential statistics to test the hypotheses. While simple percentages, mean and standard deviation were employed to describe some aspect of the data, the independent samples t-test was performed to test whether there were significant differences in mean scores between the treatment community and the control community at both baseline and after peer education intervention.
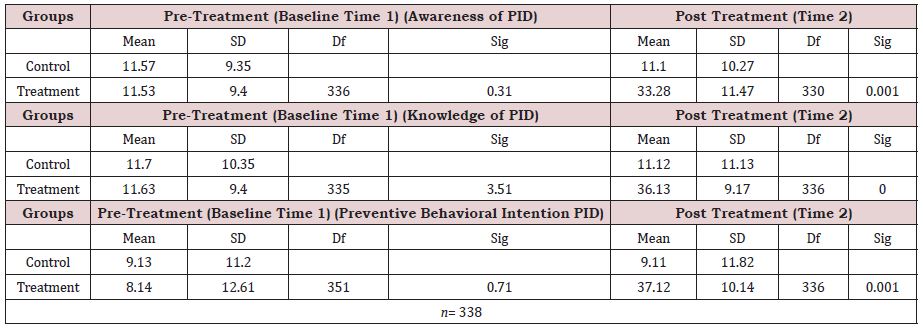
As shown in Table 1 finding for both pre-intervention and post intervention were presented to show the effect of peer education about PID on awareness of PID among women in rural communities. At the baseline, finding showed that there was no significant difference in scores for the treatment and control communities. A closer look at the mean scores also suggests that awareness about PID was particularly low. This is an indication that both communities did not significantly differ prior to being exposed to peer education intervention. However, upon intervention at time 2, findings revealed that the p value reached statistical significance. In other words, there was a significant difference in the awareness of PID for both communities. A further look at the mean scores showed that there was an improvement in the awareness level of the community exposed to information about PID through peer education intervention relative to the community that was exposed to other type of information. This outcome as shown in the table supports our first hypothesis that ‘Peer group education intervention will be effective in creating awareness on PID among rural communities.’
Further to this, the study continued by comparing results from both baseline (Time 1) and post-intervention (Time 2) in terms of knowledge level of PID for both treatment and control communities. The Finding showed that there was no statistically significant difference in the mean scores for both groups with regards to their knowledge level of PID at baseline. Both communities had low mean scores with respect to knowledge level of PID. This suggests that both communities did not differ significantly before intervention. The study also sought to determine the effect of peer education intervention on knowledge level of PID among the women who were studied post intervention. The finding revealed that there was a statistically significant difference in the knowledge of PID for women in the treatment and control community. As a result, the finding is an indication that exposure to appropriate information through peer education efforts might lead to an improvement in rural women’s knowledge of PID. Therefore, this result is in support of our second hypothesis suggesting that ‘Peer group education intervention will be effective in improving the knowledge level of PID among rural communities.’
Moreover, results from both times (1and2) were compared with regards to the rural women’s preventive behavioral intentions towards PID for those who were exposed to peer education intervention and those who were not. At the baseline, finding showed that there was no significant difference in preventive behavioral intentions scores for both treatment and control communities. Nonetheless, there was a significant difference in rural women preventive behavioral intentions mean scores of both groups at the post intervention level. More specifically, the community that was exposed to peer education program on PID improved in their preventive behavioral intentions towards PID relative to the control group who were not exposed to such intervention. This outcome attests to the likely effect peer education intervention on PID prevention might have on rural women who don’t have access to common information platforms where PID issues are disseminated. This result therefore supports our third hypothesis stating that: ‘Peer group education intervention will be effective in improving preventive behavioral intentions against PID development among rural communities.’
DISCUSSION
This study examined the effectiveness of Peer group education intervention on awareness, knowledge and preventive behavioral intentions towards PID among women in rural communities. Findings from our analyzed data support all our hypotheses in the study. More specifically, we observed that while both control and treatment communities reported low awareness and knowledge of PID at the baseline, post intervention results indicated an improvement in the awareness, knowledge and preventive behavioral intentions of women in the treatment community. As a result, we believe that peer education intervention informing women about PID could increase their awareness, knowledge and preventive behavior regarding the disease as it were. These findings are consistent with previous studies [2,6,9,10] which have highlighted the effect of peer education intervention in improving awareness, knowledge preventive practices against sexually transmitted infections across different samples. As an example, in a systematic review and meta-analysis carried out by Medley et al. [8] found that majority of the studies undertaken in developing societies, reported that peer education intervention efforts were effective especially at improving HIV knowledge and preventive behavioral outcomes relative to biological outcomes. Our findings therefore extend previous knowledge by showing that peer education intervention could be useful in reducing the rate of PID and improving the outcomes for women who are already at risk or have even contracted the disease. This is important considering the fact that PID is less of a focus compared to other common STIs like HIV and AIDS, gonorrhea, Chlamydia, Syphilis, etc. for researchers in the field of sexual health. Our result is also an indication that peer group education intervention is a potential cost-effective approach that could be employed in a developing society, especially in rural communities where women have limited access to crucial sexual health information on traditional media such as TV, radio, magazine and newspaper. Such a cost-effective approach could fill gaps left by high level illiteracy and inadequate community health workers who should be educating the women about this kind of disease and the likes.
In all, the findings from our present study have enormous implication for healthcare delivery among women in rural communities as it shows the important role peer education intervention could play in improving awareness, knowledge and preventive behavioral intentions towards PID. As earlier stated, this could serve as a cost-effective approach for addressing STIs challenges for women in these areas. Finally, the findings bring to the fore, the need for researchers and sexual health interventionists to use peer education intervention in addressing sexual health issues in rural areas where there is limited access to information platforms (i.e., traditional and modern media) despite the growing acceptance of modern media in towns and cities sharing proximity with these rural communities [11-14].
CONCLUSION
Based on the findings of this study we conclude that peer group education intervention could serve as an effective pathway to improving awareness, knowledge and behavioral intentions about PID among women in rural communities. Because PID issues do not draw as much scholarly attention as other STIs in literature, there is a great need to begin to focus on the disease that is silently affecting a number of women of childbearing everywhere. It is also imperative that we begin to find cost effective methods of disseminating necessary information that could improve preventive behavior against the disease. As a result, we recommend that, community health workers should employ peer group education approach in raising awareness, improving knowledge and encouraging preventive behavior against PID among women rural communities. When peer educators or leaders are regularly trained on PID and other STIs issues, they could start to educate other women and their friends on how to stay protected. Also, when designing the curriculum for such health education, attention should be focused on women’s sexual experiences. By understanding the categories of their sexual experiences, peer educators might begin to use this to educate more of those who are more vulnerable to the disease. Just like any other research endeavor, this study is not without its limitation. First, the study did not incorporate how the demographic variables of the women could have impacted on the results. Similarly, the study was focused singly on women in rural areas. We believe that women who have higher access to sexual health information through the Internet, TV, magazines; etc. in urban settlements could provide a better comparative basis for what we have found so far. We encourage further research efforts to address these limitations. Nevertheless, the present study has provided crucial evidence for understanding the effectiveness of peer education in promoting safe preventive practices against such STIs as PID.
REFERENCES
- Ezeah G, Ogechi EO (2020) Measuring the effect of interpersonal communication on awareness and knowledge of COVID-19 among rural communities in Eastern Nigeria. Health Education Research 35(5): 481- 489.
- Adeomi AA, Adeoye OA (2014) Evaluation of the effectiveness of peer education in improving HIV knowledge, attitude and sexual behaviors among in school Adolescents in Osun State, Nigeria. AIDS Research and Treatment 1-11.
- Bulduk S, Erdogan S (2011) The effects of peer education on reduction of the HIV/Sexually transmitted infection risk behaviors among Turkish university students. Journal of Association of Nurses in AIDS Care 23(3): 233-243.
- Ness RB, Randall H (2004) Condom use and the risk of recurrent pelvic inflammatory disease, chronic pelvic pain, or infertility following an episode of pelvic inflammatory disease. American Journal of Public Health 94(8): 1327-1329.
- Wong T, Pharr JR (2018) Effects of peer sexual health education on college campuses: A systematic review. Health Promotion Practice 20(5): 652-666.
- Jemmott JB, Jemmott LS (2015) HIV/STI risk-reduction intervention efficacy with South African adolescents over 54 months. Health Psychol 34(6): 610.
- Norr K, Tlou S (2004) Impact of peer group education on HIV prevention among women in Botswana. Health Care for Women International 25(3): 210-226.
- Medley A, Kennedy C (2009) Effectiveness of peer education interventions for HIV prevention in developing countries: A systematic review and meta-analysis. AIDS Education and Prevention 21(3): 181- 206.
- Agha S, Van Rossem R (2004) Impact of a school-based peer sexual health intervention on normative beliefs, risk perceptions, and sexual behavior of Zambian adolescents. Journal of Adolescent Health 34(5): 441-452.
- Elsayed AA, Fadel EA (2019) An educational intervention for university female students to raise sexually transmitted diseases awareness. IOSR Journal of Nursing and Health Science (IOSR-JNHS) 8(6): 39-45.
- Braun RA, Provost JM (2010) Bridging the gap: Using school-based health services to improve chlamydia screening among young women. American Journal of Public Health 100(9): 1624-1629.
- Faul F, Erdfelder E (2009) Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behavior Research Methods 41(4): 1149-1160.
- Oseni TIA, Odewale ME (2017) Socioeconomic status of parents and the occurrence of pelvic inflammatory disease among undergraduates attending Irrua Specialist Teaching Hospital, Irrua, Edo State, Nigeria. Nigerian Postgraduate Medical Journal 24(2): 114-120.
- Siddiqui M, Kataria I (2020) A systematic review of the evidence on peer education programmes for promoting the sexual and reproductive health of young people in India. Sexual and Reproductive Health Matters 28(1): 1741494.
Article Type
Research Article
Publication history
Received Date: January 21, 2022
Published: March 04, 2022
Address for correspondence
Chioma Njoku, Department of Mass Communication, University of Nigeria, Nigeria
Copyright
©2022 Open Access Journal of Biomedical Science, All rights reserved. No part of this content may be reproduced or transmitted in any form or by any means as per the standard guidelines of fair use. Open Access Journal of Biomedical Science is licensed under a Creative Commons Attribution 4.0 International License
How to cite this article
Chioma N, Luke IA. A Peer Group Education Intervention to Improve Awareness, Knowledge and Preventive Behavioral Intentions for Pelvic Inflammatory Disease (PID) Among Rural Communities in South-Eastern Nigeria. 2022- 4(2) OAJBS.ID.000408.